Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Essentials of Human Anatomy and Physiology: Chapter 10: The Endocrine SystemDocumento35 pagineEssentials of Human Anatomy and Physiology: Chapter 10: The Endocrine Systemİsmail ŞimşekNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Medical MCQ Center Liver Mcqs For Mccee Aipgmee Pgiee Jipmer Fmge State PG EntranceDocumento3 pagineMedical MCQ Center Liver Mcqs For Mccee Aipgmee Pgiee Jipmer Fmge State PG EntranceBanu KubendiranNessuna valutazione finora
- (Arun J. Sanyal, Vijay H. Shah) Portal Hypertensio (BookFi) PDFDocumento513 pagine(Arun J. Sanyal, Vijay H. Shah) Portal Hypertensio (BookFi) PDFSilvia FakhrunnisaNessuna valutazione finora
- Essentials of Anatomy and Physiology: Chapter 7: Muscular SystemDocumento9 pagineEssentials of Anatomy and Physiology: Chapter 7: Muscular Systemİsmail ŞimşekNessuna valutazione finora
- Liver AnatomyDocumento56 pagineLiver AnatomySahir100% (1)
- Clinical Embriology and Anatomy of Gi Tract Part1Documento44 pagineClinical Embriology and Anatomy of Gi Tract Part1trianaamalia100% (1)
- Blood Supply of The GITDocumento66 pagineBlood Supply of The GITgtaha80Nessuna valutazione finora
- Hemochromatosis: IntroductionDocumento10 pagineHemochromatosis: IntroductionOsamak9100% (1)
- Sinelnikov - Atlas of Human Anatomy - Volume 2 - Part 2Documento217 pagineSinelnikov - Atlas of Human Anatomy - Volume 2 - Part 2İsmail Şimşek0% (1)
- Sinelnikov - Atlas of Human Anatomy - Volume 2 - Part 2Documento217 pagineSinelnikov - Atlas of Human Anatomy - Volume 2 - Part 2İsmail Şimşek0% (1)
- Portal Hypertension PDFDocumento12 paginePortal Hypertension PDFissam_1994Nessuna valutazione finora
- Biochimie MetabolismDocumento2 pagineBiochimie MetabolismSaca AnastasiaNessuna valutazione finora
- Atlas de Anatomie A Omului McMinnDocumento340 pagineAtlas de Anatomie A Omului McMinnoana_4u_89702495% (110)
- Sinelnikov Vol 1Documento437 pagineSinelnikov Vol 1Freezy Frizzle94% (98)
- Ch27 Urinary SystemDocumento52 pagineCh27 Urinary Systemİsmail ŞimşekNessuna valutazione finora
- Human Anatomy,: First Edition Mckinley & O'LoughlinDocumento65 pagineHuman Anatomy,: First Edition Mckinley & O'Loughlinİsmail ŞimşekNessuna valutazione finora
- 25Documento41 pagine25dewkmcNessuna valutazione finora
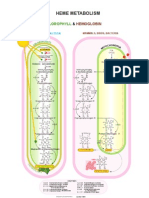
- 33 Heme MetabolismDocumento1 pagina33 Heme Metabolismİsmail ŞimşekNessuna valutazione finora
- BIOL226Lec09 - Abdominal VesselsDocumento99 pagineBIOL226Lec09 - Abdominal Vesselsİsmail ŞimşekNessuna valutazione finora
- 38 Metabolic Pathways 2Documento1 pagina38 Metabolic Pathways 2İsmail ŞimşekNessuna valutazione finora
- 28 Folic Acid C1 PoolDocumento1 pagina28 Folic Acid C1 Poolİsmail ŞimşekNessuna valutazione finora
- 27 Calvin CycleDocumento1 pagina27 Calvin Cycleİsmail ŞimşekNessuna valutazione finora
- 22 Pentose Phosohate Pathways 2Documento1 pagina22 Pentose Phosohate Pathways 2İsmail ŞimşekNessuna valutazione finora
- Acute Liver Failure-1Documento40 pagineAcute Liver Failure-1elizabethNessuna valutazione finora
- Chapter 33 - Hepatic Physiology & Amp AnesthesiaDocumento20 pagineChapter 33 - Hepatic Physiology & Amp AnesthesiaOlivia SuttonNessuna valutazione finora
- Portal HypertensionDocumento18 paginePortal Hypertensionsara82vetNessuna valutazione finora
- 2021 - Evaluation of Liver Histopathological Findings of COVID-19 by Minimally Invasive AutopsiesDocumento24 pagine2021 - Evaluation of Liver Histopathological Findings of COVID-19 by Minimally Invasive AutopsiesMario Martínez TorijaNessuna valutazione finora
- Blood Vessels Review SheetDocumento6 pagineBlood Vessels Review Sheet9Speed93% (14)
- 3-Major Veins of The BodyDocumento26 pagine3-Major Veins of The BodyTJPlayz100% (1)
- Abdominal OrgansDocumento132 pagineAbdominal OrgansSheryl Layne LaoNessuna valutazione finora
- Liver Transplant Workup: IntroductionDocumento9 pagineLiver Transplant Workup: IntroductionKay BristolNessuna valutazione finora
- ESR Ebook For Undergraduate Education in Radiology - 08a Liver Imaging PDFDocumento80 pagineESR Ebook For Undergraduate Education in Radiology - 08a Liver Imaging PDFANAS ALINessuna valutazione finora
- VaricesDocumento34 pagineVaricesapi-19641337Nessuna valutazione finora
- Cirrhosis of The Liver Nursing Care Management Symptoms NCLEXDocumento10 pagineCirrhosis of The Liver Nursing Care Management Symptoms NCLEXParallelNessuna valutazione finora
- Anatomy Liver, Biliary, Pancreas and Spleen 2022Documento58 pagineAnatomy Liver, Biliary, Pancreas and Spleen 2022Osama AbdelazizNessuna valutazione finora
- Hypertension CaseDocumento3 pagineHypertension CaseArnold Christian QuilonNessuna valutazione finora
- Compare The Pulmonary and Systemic Circuits of The Cardiovascular SystemDocumento6 pagineCompare The Pulmonary and Systemic Circuits of The Cardiovascular Systememanuel coatesNessuna valutazione finora
- Blood Supply of Whole BodyDocumento60 pagineBlood Supply of Whole BodyProsanjit Majumder100% (1)
- Cholangiocarcinoma Case StudyDocumento19 pagineCholangiocarcinoma Case Studyapi-349474075Nessuna valutazione finora
- Rounds: Case Study and Review of Autoimmune HepatitisDocumento7 pagineRounds: Case Study and Review of Autoimmune HepatitisClaudia Naomi Ventura OrtizNessuna valutazione finora
- Liver Anatomy - SnellDocumento2 pagineLiver Anatomy - SnelltristineNessuna valutazione finora
- Liver Blood FlowDocumento4 pagineLiver Blood Flowhomam Salim Khalaf100% (1)
- Portal HypertensionDocumento46 paginePortal HypertensionalcaponeNessuna valutazione finora
- Anatomi CT Scan AbdomenDocumento17 pagineAnatomi CT Scan Abdomenwawan saifullahNessuna valutazione finora
- Hepatobiliary System-Anatomy & PhysiologyDocumento49 pagineHepatobiliary System-Anatomy & PhysiologyDeshi SportsNessuna valutazione finora
- Human Biochem MuscDocumento408 pagineHuman Biochem MuscMa Anna Cris LumongsudNessuna valutazione finora