Potrebbero piacerti anche
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1091)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Chapter End Stop SignsDocumento4 pagineChapter End Stop Signsapi-307327939Nessuna valutazione finora
- Breast UltrasoundDocumento57 pagineBreast UltrasoundYoungFanjiensNessuna valutazione finora
- Goodbye HachikoDocumento6 pagineGoodbye HachikoAbraham LizardoNessuna valutazione finora
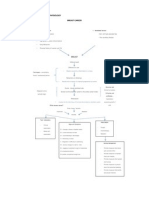
- Etiology and Pathophysiology Breast CancerDocumento1 paginaEtiology and Pathophysiology Breast Cancermay_hisolerNessuna valutazione finora
- Drug Study Format Ready To PrintDocumento2 pagineDrug Study Format Ready To Printmay_hisolerNessuna valutazione finora
- AutoSPRINK12InstallationWalkthrough PDFDocumento2 pagineAutoSPRINK12InstallationWalkthrough PDFHai PhamNessuna valutazione finora
- Design Aeroleaf Wind Turbine PDFDocumento98 pagineDesign Aeroleaf Wind Turbine PDFananduNessuna valutazione finora
- Discharge Plan: MedicationDocumento2 pagineDischarge Plan: Medicationmay_hisolerNessuna valutazione finora
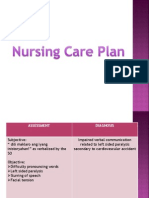
- NCP CvaDocumento7 pagineNCP Cvamay_hisolerNessuna valutazione finora
- Miyat PresentationDocumento73 pagineMiyat Presentationmay_hisolerNessuna valutazione finora
- Breast CompositionDocumento1 paginaBreast Compositionmay_hisolerNessuna valutazione finora
- Miyat PresentationDocumento73 pagineMiyat Presentationmay_hisolerNessuna valutazione finora
- CuesDocumento2 pagineCuesmay_hisolerNessuna valutazione finora
- Card It IsDocumento3 pagineCard It Ismay_hisolerNessuna valutazione finora
- Black Box Testing TechniquesDocumento28 pagineBlack Box Testing TechniquesAshish YadavNessuna valutazione finora
- 10th Triple Helix Conference 2012 University, Industry, and Government Partnership: Its Present and Future Challenges in IndonesiaDocumento10 pagine10th Triple Helix Conference 2012 University, Industry, and Government Partnership: Its Present and Future Challenges in IndonesiaMery Citra SondariNessuna valutazione finora
- System Analysis & Design: Structuring System Process RequirementsDocumento52 pagineSystem Analysis & Design: Structuring System Process RequirementsNusrat Jahan NafisaNessuna valutazione finora
- North West Karnataka Road Transport Corporation: (Application For Student Bus Pass)Documento3 pagineNorth West Karnataka Road Transport Corporation: (Application For Student Bus Pass)RasoolkhanNessuna valutazione finora
- Remote Digital Input (Rdi-32Xe / Rdi-32Axe) : Distributed Processing UnitsDocumento2 pagineRemote Digital Input (Rdi-32Xe / Rdi-32Axe) : Distributed Processing UnitsCHAIRMANNessuna valutazione finora
- Bending Tools RF-A English - OriginalDocumento116 pagineBending Tools RF-A English - OriginalGunnie PandherNessuna valutazione finora
- Fruit CakeDocumento3 pagineFruit CakeCynthia OnuigboNessuna valutazione finora
- Grandfather Tang Lesson PlanDocumento6 pagineGrandfather Tang Lesson PlanalyssamanningNessuna valutazione finora
- 4TH Quarter Grade 9 Pe Learning Activity Sheets Week 1 4 1Documento15 pagine4TH Quarter Grade 9 Pe Learning Activity Sheets Week 1 4 1Kelvin Pastor EncarnacionNessuna valutazione finora
- Talcott ParsonsDocumento20 pagineTalcott Parsonssyedarida fatimaNessuna valutazione finora
- Honeywell Question 1&2Documento6 pagineHoneywell Question 1&2anon_909027967Nessuna valutazione finora
- Black 2018 B Uploaded VersionDocumento46 pagineBlack 2018 B Uploaded VersionOwais AhmedNessuna valutazione finora
- EUCR-W 2009 - Captains PackDocumento9 pagineEUCR-W 2009 - Captains Packapi-16087835Nessuna valutazione finora
- SHPB2012 Barras de Cromsteel PDFDocumento24 pagineSHPB2012 Barras de Cromsteel PDFEdgar Rojas EspejoNessuna valutazione finora
- G Schock G-2210 ManualDocumento2 pagineG Schock G-2210 ManualcaquirinoNessuna valutazione finora
- CAF 8 AUD Autumn 2022Documento3 pagineCAF 8 AUD Autumn 2022Huma BashirNessuna valutazione finora
- Xtreet 250X 2017 Parts Catalogue 2016 08 16 1Documento32 pagineXtreet 250X 2017 Parts Catalogue 2016 08 16 1JeovannyAlexanderMatamorosSanchezNessuna valutazione finora
- Multiple Choice Quiz Chapter 5Documento4 pagineMultiple Choice Quiz Chapter 5gottwins05Nessuna valutazione finora
- Title 250706Documento556 pagineTitle 250706callmeasthaNessuna valutazione finora
- Paper171 I.banuDocumento6 paginePaper171 I.banuIoan-Viorel BanuNessuna valutazione finora
- R 2 KyDocumento3 pagineR 2 KyJorge AzurduyNessuna valutazione finora
- Autoplant TutorialDocumento404 pagineAutoplant TutorialManish Tukaram Deshpande100% (1)
- Comparison... Lesson PlanDocumento4 pagineComparison... Lesson PlanHicham EljarrariNessuna valutazione finora
- R2900G JLK01211 ConfigurationDocumento2 pagineR2900G JLK01211 Configurationjc villongcoNessuna valutazione finora
- Individual AssignmentDocumento17 pagineIndividual AssignmentYousef AboamaraNessuna valutazione finora