Potrebbero piacerti anche
- Problem-based Approach to Gastroenterology and HepatologyDa EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNessuna valutazione finora
- Lung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesDa EverandLung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesAlain JunodNessuna valutazione finora
- Newborn EmergenciesDocumento83 pagineNewborn EmergencieshwelpNessuna valutazione finora
- Pediatric Cardiology and Pulmonology: A Practically Painless ReviewDa EverandPediatric Cardiology and Pulmonology: A Practically Painless ReviewNessuna valutazione finora
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsDa EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNessuna valutazione finora
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsDa EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNessuna valutazione finora
- 14 Fun Facts About Your Heart: Educational VersionDa Everand14 Fun Facts About Your Heart: Educational VersionNessuna valutazione finora
- Respiratory Failure (KK 2a)Documento29 pagineRespiratory Failure (KK 2a)IlaJako StefanaticNessuna valutazione finora
- Wolff-Parkinson- White-Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandWolff-Parkinson- White-Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Pulmonary Function Test, JARA CSUDocumento73 paginePulmonary Function Test, JARA CSUJohn NicoleNessuna valutazione finora
- Critical Thinking in Respiratory Care Practice PDFDocumento17 pagineCritical Thinking in Respiratory Care Practice PDFFernando MorenoNessuna valutazione finora
- Anaerobic Infections in HumansDa EverandAnaerobic Infections in HumansSydney FinegoldValutazione: 5 su 5 stelle5/5 (1)
- 66 Neonatal Resuscitation Show Notes 1Documento3 pagine66 Neonatal Resuscitation Show Notes 1Rabbani IcksanNessuna valutazione finora
- Community-Acquired Pneumonia: Strategies for ManagementDa EverandCommunity-Acquired Pneumonia: Strategies for ManagementAntoni TorresValutazione: 4.5 su 5 stelle4.5/5 (2)
- RespiratoryDocumento161 pagineRespiratoryDanity_Anne_Ba_1326100% (1)
- ICU Scoring Systems A Complete Guide - 2020 EditionDa EverandICU Scoring Systems A Complete Guide - 2020 EditionNessuna valutazione finora
- Respiratory Acidosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandRespiratory Acidosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Congenital Anomalies of Airway and Lung ParenchymaDocumento71 pagineCongenital Anomalies of Airway and Lung ParenchymaGopal ChawlaNessuna valutazione finora
- Lung Development Biological and Clinical Perspectives: Biochemistry and PhysiologyDa EverandLung Development Biological and Clinical Perspectives: Biochemistry and PhysiologyPhilip FarrellNessuna valutazione finora
- Respiratory PhysiologyDocumento16 pagineRespiratory PhysiologyYsabel Salvador DychincoNessuna valutazione finora
- Respiratory PathophysDocumento1 paginaRespiratory PathophysTori IkeharaNessuna valutazione finora
- CXR Lecture DR Lenora FernandezDocumento70 pagineCXR Lecture DR Lenora Fernandezapi-19431894100% (1)
- Cardiovascular Pathology 1:: Blood VesselsDocumento48 pagineCardiovascular Pathology 1:: Blood VesselsRaiver CadenNessuna valutazione finora
- Registry Examination For Advanced Respiratory Therapists (RRT)Documento6 pagineRegistry Examination For Advanced Respiratory Therapists (RRT)Sandy HartmanNessuna valutazione finora
- Atelectasis, (Lung Collapse) A Simple Guide To The Condition, Diagnosis, Treatment And Related DiseasesDa EverandAtelectasis, (Lung Collapse) A Simple Guide To The Condition, Diagnosis, Treatment And Related DiseasesNessuna valutazione finora
- Cardiac Tamponade, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandCardiac Tamponade, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Hereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandHereditary Spherocytosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- HFOV High-Frequency-Oscillatory-VentilationDocumento22 pagineHFOV High-Frequency-Oscillatory-VentilationJZNessuna valutazione finora
- Respiratory Alkalosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandRespiratory Alkalosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Acute Respiratory Distress Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandAcute Respiratory Distress Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- PericarditisDocumento29 paginePericarditisPavin KumarNessuna valutazione finora
- Registered Respiratory TherapistDocumento3 pagineRegistered Respiratory Therapistapi-76909521Nessuna valutazione finora
- Prematurity: DR - Azhar Hamza AlsaqyDocumento18 paginePrematurity: DR - Azhar Hamza AlsaqyChro MANessuna valutazione finora
- Respiratory EmergenciesDocumento34 pagineRespiratory EmergenciesRoshana MallawaarachchiNessuna valutazione finora
- Pediatric Mechanical VentilationDocumento49 paginePediatric Mechanical VentilationNirubhana ArunthavasothyNessuna valutazione finora
- Mechanical Ventilation and Intracranial PressureDocumento30 pagineMechanical Ventilation and Intracranial PressureFlavius AnghelNessuna valutazione finora
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsDa EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsNessuna valutazione finora
- Mechanical VentDocumento24 pagineMechanical VentRochim CoolNessuna valutazione finora
- The Lung Circulation: Physiology and PharmacologyDa EverandThe Lung Circulation: Physiology and PharmacologyNessuna valutazione finora
- Congenital Heart Diseases, A Simple Guide to these Medical ConditionsDa EverandCongenital Heart Diseases, A Simple Guide to these Medical ConditionsNessuna valutazione finora
- Pediatric EmergenciesDocumento79 paginePediatric Emergenciesأحمد سعد الديوه جيNessuna valutazione finora
- RespiratoryDocumento4 pagineRespiratoryHaliana IzatiNessuna valutazione finora
- Mnemonic SDocumento78 pagineMnemonic SJoevet T. TadlasNessuna valutazione finora
- John PFTDocumento231 pagineJohn PFTAlexander Santiago ParelNessuna valutazione finora
- AA GradientDocumento2 pagineAA GradientzaminazzNessuna valutazione finora
- Pediatric Asthma PDFDocumento12 paginePediatric Asthma PDFzie_luph_taz13Nessuna valutazione finora
- Newborn ExaminationDocumento45 pagineNewborn ExaminationHamka HamNessuna valutazione finora
- 161111163114Documento31 pagine161111163114lejizixNessuna valutazione finora
- DR Johnson On Neonatal Resuscitation Guidelines 041707Documento44 pagineDR Johnson On Neonatal Resuscitation Guidelines 041707sameerarswNessuna valutazione finora
- Congenital Heart DiseasesDocumento52 pagineCongenital Heart DiseasesCristina Maria100% (1)
- Distributive Shock 1Documento41 pagineDistributive Shock 1Fuzi HannyNessuna valutazione finora
- Trachs, Vents, and Passy-MuirDocumento30 pagineTrachs, Vents, and Passy-MuirCharles S. Williams RRT, AE-C100% (4)
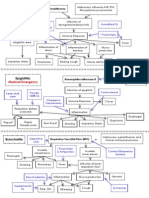
- Lung Pathology Flow ChartsDocumento6 pagineLung Pathology Flow ChartsZagros MotamedNessuna valutazione finora
- Breathing and Exchange of GasesDocumento5 pagineBreathing and Exchange of Gaseslpc4944Nessuna valutazione finora
- Respiratory PathophysDocumento1 paginaRespiratory PathophysTori IkeharaNessuna valutazione finora
- Persistent Pulmonary Hypertension in Newborn: By: Dr. Abhay Kumar Moderator: Dr. Akhilesh KumarDocumento31 paginePersistent Pulmonary Hypertension in Newborn: By: Dr. Abhay Kumar Moderator: Dr. Akhilesh KumarAbhay BarnwalNessuna valutazione finora
- Physiology of VomitingDocumento24 paginePhysiology of VomitingKingWayne Tagatac BajoNessuna valutazione finora
- Polycythemia in NewbornDocumento25 paginePolycythemia in NewbornTheva Thy100% (2)
- Hypertension: Kieran Mcglade Nov 2001 Department of General Practice QubDocumento25 pagineHypertension: Kieran Mcglade Nov 2001 Department of General Practice QubTheva ThyNessuna valutazione finora
- Maxwell Quick Medical Reference PDFDocumento35 pagineMaxwell Quick Medical Reference PDFAnonymous fj68Ms100% (10)
- Approach To The Adult Patient With Fever of Unknown OriginDocumento6 pagineApproach To The Adult Patient With Fever of Unknown Origini can always make u smile :D100% (1)
- 2 Challenges To Medical Students Tan Sri Dato' Seri DR HJ Mohd Ismail MericanDocumento4 pagine2 Challenges To Medical Students Tan Sri Dato' Seri DR HJ Mohd Ismail MericanTheva ThyNessuna valutazione finora
- Final Thesis 2018 08 23 18 13 33 319 PDFDocumento69 pagineFinal Thesis 2018 08 23 18 13 33 319 PDFPriyanka KanodiaNessuna valutazione finora
- Peds Restorative PDFDocumento4 paginePeds Restorative PDFmirfanulhaqNessuna valutazione finora
- Bedpans and UrinalsDocumento4 pagineBedpans and UrinalsCham De Leon50% (4)
- Name: Ma. Princess P. Seril DATE: DECEMBER 5, 6, 8, 9-2011 GROUP: 53 Area: Alimannao Rhu Clinical Instructor: Evelyn C. Cristobal, RNDocumento2 pagineName: Ma. Princess P. Seril DATE: DECEMBER 5, 6, 8, 9-2011 GROUP: 53 Area: Alimannao Rhu Clinical Instructor: Evelyn C. Cristobal, RNRoshin TejeroNessuna valutazione finora
- Evaluating Information Systems PDFDocumento373 pagineEvaluating Information Systems PDFDwi Nur Amalia0% (1)
- Appendix and Cecum!Documento13 pagineAppendix and Cecum!SilvanaPutriNessuna valutazione finora
- Alcoholic Liver DiseaseDocumento8 pagineAlcoholic Liver DiseaseCassandra ZubeheourNessuna valutazione finora
- Ceramic Inlays A Case Presentation and LessonsDocumento11 pagineCeramic Inlays A Case Presentation and LessonsStef David100% (1)
- Curahealth Hospitals Completes The Purchase of Specialty Hospital of JacksonvilleDocumento2 pagineCurahealth Hospitals Completes The Purchase of Specialty Hospital of JacksonvillePR.comNessuna valutazione finora
- Adult Congenital Heart Disease - Cardiovascular Medicine - MKSAP 17Documento13 pagineAdult Congenital Heart Disease - Cardiovascular Medicine - MKSAP 17alaaNessuna valutazione finora
- Thuasne Practical Guide 2005Documento23 pagineThuasne Practical Guide 2005arya091193Nessuna valutazione finora
- Welch Allyn Pic 30 Manual ServicioDocumento147 pagineWelch Allyn Pic 30 Manual ServicioPaola Del CairoNessuna valutazione finora
- AphasiaDocumento45 pagineAphasiaHenry SugihartoNessuna valutazione finora
- Sops Medical Office Survey: Language: EnglishDocumento8 pagineSops Medical Office Survey: Language: EnglishRiana MarsellaNessuna valutazione finora
- Drug Study ProjectDocumento7 pagineDrug Study ProjectMaRic Gabutin Guerra100% (1)
- 1 s2.0 S1879729618300073 MainDocumento5 pagine1 s2.0 S1879729618300073 MainAditiya RonaldiNessuna valutazione finora
- NCLEX-Copy of 336 Questions With AnswersDocumento336 pagineNCLEX-Copy of 336 Questions With AnswersYanah100% (21)
- A House Officer's Approach To DengueDocumento9 pagineA House Officer's Approach To DengueBaihaqi SaharunNessuna valutazione finora
- HCFA 2007 Annual ReportDocumento20 pagineHCFA 2007 Annual ReportHCFAMANessuna valutazione finora
- NCP Impaired Skintissue IntegrityDocumento5 pagineNCP Impaired Skintissue IntegrityArt Christian RamosNessuna valutazione finora
- Nclex Questions: 70Documento17 pagineNclex Questions: 70RJ MarthewNessuna valutazione finora
- Codman's Paradox in Adhesive Capsulitis: StudyDocumento3 pagineCodman's Paradox in Adhesive Capsulitis: StudyHari25885Nessuna valutazione finora
- ACUTE RESPIRATORY FAILURE QuizDocumento3 pagineACUTE RESPIRATORY FAILURE QuizTrish 001950% (2)
- Orthopaedics Guide - 2009Documento31 pagineOrthopaedics Guide - 2009IMNessuna valutazione finora
- MaxalonDocumento7 pagineMaxalonran manaliliNessuna valutazione finora
- The Color of Rain by Michael and Gina SpehnDocumento26 pagineThe Color of Rain by Michael and Gina SpehnZondervan100% (1)
- Blood Circulation QuestionsDocumento2 pagineBlood Circulation QuestionsMiran El-MaghrabiNessuna valutazione finora
- NFDN 2003 Report On Progress of Professional PortfolioDocumento2 pagineNFDN 2003 Report On Progress of Professional Portfolioapi-318575574Nessuna valutazione finora
- InstructionDocumento13 pagineInstructionstealth8678Nessuna valutazione finora
- Mu CostaDocumento6 pagineMu Costafarracholidia_867630Nessuna valutazione finora