Potrebbero piacerti anche
- Approach To A Patient With Acute Kidney InjuryDocumento70 pagineApproach To A Patient With Acute Kidney InjuryShivamNessuna valutazione finora
- IKD6 - Contrast Associated AKIDocumento44 pagineIKD6 - Contrast Associated AKIRenal Association MauritiusNessuna valutazione finora
- Acute Kidney InjuryDocumento64 pagineAcute Kidney InjuryBIAN ALKHAZMARINessuna valutazione finora
- Murray CaseStudiesInNephrologyDocumento179 pagineMurray CaseStudiesInNephrologyAdil BilaeloNessuna valutazione finora
- Contrast Induced NephropathyDocumento25 pagineContrast Induced NephropathyXin Yee TanNessuna valutazione finora
- Peripheral Vascular Diseases - FinalDocumento48 paginePeripheral Vascular Diseases - FinalBibek GhimireNessuna valutazione finora
- Neutropenic Sepsis-Tls-Anaphylaxis-ExtravasationDocumento40 pagineNeutropenic Sepsis-Tls-Anaphylaxis-ExtravasationSA NodeNessuna valutazione finora
- Anaesthesia For Post TA HemorrhageDocumento31 pagineAnaesthesia For Post TA HemorrhageNovus LeoNessuna valutazione finora
- L11 Renal Failure General Approach 230213 002819Documento16 pagineL11 Renal Failure General Approach 230213 002819S sNessuna valutazione finora
- Acute Kidney InjuryDocumento44 pagineAcute Kidney InjurySuci MayveraNessuna valutazione finora
- Tubulopathies. Interstitial NephritisDocumento34 pagineTubulopathies. Interstitial NephritisIaros OlgaNessuna valutazione finora
- Acute Kidney Injury AKIDocumento6 pagineAcute Kidney Injury AKIfazeel shah vlogsNessuna valutazione finora
- Anaesthesia For Renal TransplantationDocumento65 pagineAnaesthesia For Renal TransplantationSouvik MaitraNessuna valutazione finora
- Acute Kidney InjuryDocumento34 pagineAcute Kidney Injury* mokhtar !!Nessuna valutazione finora
- Acute Kidney Injury:: A Brief OutlineDocumento48 pagineAcute Kidney Injury:: A Brief OutlinehanaNessuna valutazione finora
- HRSDocumento63 pagineHRSPriya KalariaNessuna valutazione finora
- Material For Cme - AKIDocumento20 pagineMaterial For Cme - AKIHzm AzizulNessuna valutazione finora
- Acute Kidney InjuryDocumento42 pagineAcute Kidney Injurymedpedshospitalist100% (1)
- Approach Nefroritic SXDocumento58 pagineApproach Nefroritic SX[ qιlα ]Nessuna valutazione finora
- 16 - RE - Acute Kidney InjuryDocumento8 pagine16 - RE - Acute Kidney Injury078229933aaNessuna valutazione finora
- Referat Hepatorenal Syndrome: Pembimbing: Dr. Sahala Panggabean SPPD KGH Presentan: Ilham Suryo Wibowo AntonoDocumento40 pagineReferat Hepatorenal Syndrome: Pembimbing: Dr. Sahala Panggabean SPPD KGH Presentan: Ilham Suryo Wibowo AntonoIlham Suryo Wibowo AntonoNessuna valutazione finora
- Acute Kidney Injury (AKI) : Departemen Penyakit DalamDocumento43 pagineAcute Kidney Injury (AKI) : Departemen Penyakit DalamFitria Dewi LestariNessuna valutazione finora
- Upper GI BleedDocumento50 pagineUpper GI BleedNiladri BanerjeeNessuna valutazione finora
- Nephrology: Omar K MRCP IrelandDocumento54 pagineNephrology: Omar K MRCP IrelandManmeet SNessuna valutazione finora
- Acute Kidney Injury and Kidney Replacement Therapy in AdultsDocumento7 pagineAcute Kidney Injury and Kidney Replacement Therapy in Adultsjsali9210Nessuna valutazione finora
- DR Stuart McPherson - Management of Decompensated CirrhosisDocumento33 pagineDR Stuart McPherson - Management of Decompensated Cirrhosisana_miulescuNessuna valutazione finora
- Drug Induced Kidney Disease: Dr. Hamid SaeedDocumento42 pagineDrug Induced Kidney Disease: Dr. Hamid SaeedKhadija KamranNessuna valutazione finora
- Gangguan Ginjal AkutDocumento29 pagineGangguan Ginjal Akutb3djo_76Nessuna valutazione finora
- Arf in Icu: James YewDocumento20 pagineArf in Icu: James Yewyewha550Nessuna valutazione finora
- C370 Lecture 1 Lecture Notes Part 2Documento54 pagineC370 Lecture 1 Lecture Notes Part 2Yan Mui ChanNessuna valutazione finora
- Abdominal TraumaDocumento39 pagineAbdominal TraumaMuvenn KannanNessuna valutazione finora
- Acute Kidney InjuryDocumento16 pagineAcute Kidney Injurylutha izzatiNessuna valutazione finora
- Lower GI BleedingDocumento28 pagineLower GI BleedingSK TalkNessuna valutazione finora
- Toronto Notes Nephrology 2015 27Documento1 paginaToronto Notes Nephrology 2015 27JUSASBNessuna valutazione finora
- Acute Kidney Injury and Chronic Kidney DiseaseDocumento44 pagineAcute Kidney Injury and Chronic Kidney DiseaseshihochanNessuna valutazione finora
- Anesthesia For Kidney DiseaseDocumento6 pagineAnesthesia For Kidney DiseaseFrits Dede SinagaNessuna valutazione finora
- Toronto Notes Nephrology 2015 33Documento1 paginaToronto Notes Nephrology 2015 33JUSASBNessuna valutazione finora
- Renal FailureDocumento48 pagineRenal FailureCindy MamalangkasNessuna valutazione finora
- Acute Kidney Failure: Dr. Syamsudin, M.Biomed Fakultas Farmasi Universitas PancasilaDocumento48 pagineAcute Kidney Failure: Dr. Syamsudin, M.Biomed Fakultas Farmasi Universitas PancasilariyuNessuna valutazione finora
- Hepatorenal Syndrome: DR Allister J Grant Leicester Liver UnitDocumento24 pagineHepatorenal Syndrome: DR Allister J Grant Leicester Liver UnitchanataliaNessuna valutazione finora
- Approach To Peripheral Vascular Diseases and Management: Shambhavi Sharma MS, 2 Year Resident PahsDocumento49 pagineApproach To Peripheral Vascular Diseases and Management: Shambhavi Sharma MS, 2 Year Resident PahsRAKSHITH M SNessuna valutazione finora
- Antico Agne Ur AxialDocumento27 pagineAntico Agne Ur AxialPraveen RamasamyNessuna valutazione finora
- Board Review: Nephrology: Wednesday, August 19Documento65 pagineBoard Review: Nephrology: Wednesday, August 19Lina Abuarqoub67% (3)
- Diabetic Nephropathyt: Benyamin S.I HutagaolDocumento28 pagineDiabetic Nephropathyt: Benyamin S.I HutagaolBen IntosiusNessuna valutazione finora
- Nephrology Review NotesDocumento6 pagineNephrology Review NotesEdilberto HernandezNessuna valutazione finora
- Etiology: 1.urinary RetentionDocumento38 pagineEtiology: 1.urinary RetentionAbdurre YNessuna valutazione finora
- Chapter 2 - C - III Portal HypertensionDocumento37 pagineChapter 2 - C - III Portal HypertensionEmmaNessuna valutazione finora
- Fulminant Hepatic Failure: 7 October 2009 Morning Report Christine Williams, MDDocumento25 pagineFulminant Hepatic Failure: 7 October 2009 Morning Report Christine Williams, MDAndreas SichoneNessuna valutazione finora
- Atul Sharma Uppergi Fcccm23Documento47 pagineAtul Sharma Uppergi Fcccm23Atul SharmaNessuna valutazione finora
- Updates On Acute Coronary SyndromeDocumento121 pagineUpdates On Acute Coronary SyndromeDwi Akbarina YahyaNessuna valutazione finora
- Renal Replacment ThearpyDocumento93 pagineRenal Replacment ThearpySabrina ShalhoutNessuna valutazione finora
- Integrated Therapeutics IiDocumento165 pagineIntegrated Therapeutics IiSalahadinNessuna valutazione finora
- MRCP 2 Nephrology NOTESDocumento74 pagineMRCP 2 Nephrology NOTESMuhammad HaneefNessuna valutazione finora
- Renal NotesDocumento11 pagineRenal NotesPatty Pasarilla Passehl100% (2)
- 15 - Policistic Kidney Disease, Acute Tubular Necrosis, Pyelonefritis AkutDocumento48 pagine15 - Policistic Kidney Disease, Acute Tubular Necrosis, Pyelonefritis Akutsalsabr21Nessuna valutazione finora
- Pedoman Tatalaksana Sindrom Koroner Akut 2015Documento29 paginePedoman Tatalaksana Sindrom Koroner Akut 2015Vittorio bagscenterNessuna valutazione finora
- 22.AKI ProtocolDocumento2 pagine22.AKI ProtocolRed DevilNessuna valutazione finora
- Renal Diseases " Review "Documento22 pagineRenal Diseases " Review "api-3827876Nessuna valutazione finora
- FLUID, ELECTROLYTE, AND ACID-BASE PHYSIOLOGY - A PROBLEM-BASED APPROACH (4E) (2010) (UnitedVRG) PDFDocumento614 pagineFLUID, ELECTROLYTE, AND ACID-BASE PHYSIOLOGY - A PROBLEM-BASED APPROACH (4E) (2010) (UnitedVRG) PDFCristinaLucan100% (2)
- Urinalysis Is A Diagnostic Physical, Chemical, and Microscopic Examination ofDocumento4 pagineUrinalysis Is A Diagnostic Physical, Chemical, and Microscopic Examination ofjadeyjadeNessuna valutazione finora
- Facts On Aging QuizDocumento22 pagineFacts On Aging QuizKadi Thomas100% (1)
- 4 HTA RenDocumento37 pagine4 HTA RenBordean LilianaNessuna valutazione finora
- Renal Cell Carcinoma Grand Case StudyDocumento81 pagineRenal Cell Carcinoma Grand Case StudyAJIgama100% (1)
- Clinical Use of Herbs & Herbal Medicine inDocumento17 pagineClinical Use of Herbs & Herbal Medicine inAhmed ImranNessuna valutazione finora
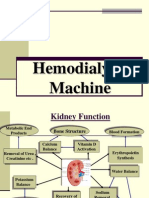
- Hemodialysis Machine12Documento45 pagineHemodialysis Machine12Divya SoundarajanNessuna valutazione finora
- Nursing Care Plan of Client With Fluid and Electrolyte ImbalanceDocumento28 pagineNursing Care Plan of Client With Fluid and Electrolyte ImbalanceCj Aguilar50% (2)
- IV FluidDocumento28 pagineIV FluidZulfkar Latief QadrieNessuna valutazione finora
- Physiology With Bioethics (2 Course)Documento29 paginePhysiology With Bioethics (2 Course)Divine ElyaNessuna valutazione finora
- Implications of The CANUSA Study PDFDocumento6 pagineImplications of The CANUSA Study PDFCarlos Navarro YslaNessuna valutazione finora
- Intestinal Sodium Glucose Cotransporter 3 Expression Is Epithe - 2021 - Life SciDocumento11 pagineIntestinal Sodium Glucose Cotransporter 3 Expression Is Epithe - 2021 - Life SciPaoloMafaldoNessuna valutazione finora
- Pex 09 01Documento5 paginePex 09 01Gerardien Elham AfifahNessuna valutazione finora
- Management of Hyperphosphatemia in End-Stage Renal Disease A New ParadigDocumento14 pagineManagement of Hyperphosphatemia in End-Stage Renal Disease A New ParadigsamuelNessuna valutazione finora
- UrinDocumento2 pagineUrinnacha nurhasanahNessuna valutazione finora
- Chronic Kidney DiseaseDocumento20 pagineChronic Kidney DiseasePappu HSD VenkateshNessuna valutazione finora
- 2nd Grading Science ReviewerDocumento10 pagine2nd Grading Science ReviewerEn CyNessuna valutazione finora
- The Normal Kidney: Pediatrics 2 The Urinary System and Urinary Tract InfectionsDocumento4 pagineThe Normal Kidney: Pediatrics 2 The Urinary System and Urinary Tract Infectionssarguss14Nessuna valutazione finora
- UralytDocumento5 pagineUralytclau_wildNessuna valutazione finora
- Renal Failure in Burn :: الفشل الكلوي لدى مرضى الحروقDocumento36 pagineRenal Failure in Burn :: الفشل الكلوي لدى مرضى الحروقDr Mohamed A. El Rouby100% (2)
- Bartter Syndrome and Gitelman SyndromeDocumento13 pagineBartter Syndrome and Gitelman Syndromelbc-602Nessuna valutazione finora
- Nephrotic Syndrome: DR Thuvaraka WareDocumento5 pagineNephrotic Syndrome: DR Thuvaraka Warechloe1411Nessuna valutazione finora
- Case Study HypertnsionDocumento32 pagineCase Study HypertnsionAnkush Kulat PatilNessuna valutazione finora
- Lab Report Exp 2 - Kidney Function & Physiology (Group 4)Documento10 pagineLab Report Exp 2 - Kidney Function & Physiology (Group 4)FARHAH BATRISYIA ABDUL RAHIMNessuna valutazione finora
- Acute Renal Failure: Presented by Peter Fumo, MD, FACPDocumento20 pagineAcute Renal Failure: Presented by Peter Fumo, MD, FACPlagathurcNessuna valutazione finora
- Boron Intrebari Pentru Evaluare enDocumento42 pagineBoron Intrebari Pentru Evaluare enAna0% (1)
- Clinical Presentation of Renal Disease: Persistent Urinary AbnormalitiesDocumento27 pagineClinical Presentation of Renal Disease: Persistent Urinary AbnormalitiesradhiinathahirNessuna valutazione finora
- Junal ScreeningDocumento9 pagineJunal ScreeningRama BayuNessuna valutazione finora
- Bibliography 1. BooksDocumento4 pagineBibliography 1. BooksJim RashidNessuna valutazione finora
- Hypertension in Hemodialysis PatientDocumento54 pagineHypertension in Hemodialysis PatientIchtiar MahesaNessuna valutazione finora