Potrebbero piacerti anche
- Super BugDocumento22 pagineSuper BugRahul NetragaonkarNessuna valutazione finora
- Children's Prayers to Thank God for His Blessings - Children's Christian Prayer BooksDa EverandChildren's Prayers to Thank God for His Blessings - Children's Christian Prayer BooksNessuna valutazione finora
- Bible Quiz Test Your Biblical Knowledge Old Testament Challenging Trivia Questions & Fun Facts for Study & Sunday School: Christian BooksDa EverandBible Quiz Test Your Biblical Knowledge Old Testament Challenging Trivia Questions & Fun Facts for Study & Sunday School: Christian BooksNessuna valutazione finora
- The Language of Care: Stories from the Penn Medicine Listening LabDa EverandThe Language of Care: Stories from the Penn Medicine Listening LabNessuna valutazione finora
- Mental Health First AidDocumento4 pagineMental Health First Aiddskubi8661Nessuna valutazione finora
- Measles Also Known As Rubeola: Shellah Zafirah E. AbantasDocumento12 pagineMeasles Also Known As Rubeola: Shellah Zafirah E. AbantasAdriana SutuNessuna valutazione finora
- BSBWOR301 Student Assessment Task 3Documento25 pagineBSBWOR301 Student Assessment Task 3Aqsa MuzammilNessuna valutazione finora
- Manual Handling: Ian Stone Health and Safety AdvisorDocumento60 pagineManual Handling: Ian Stone Health and Safety AdvisorMuhammad Syafiq Sutan ShahrilNessuna valutazione finora
- Respiratory Tract Illnesses in Pediatrics: - Classification - Detail Discussion - Diagnosis - Management - PreventionDocumento17 pagineRespiratory Tract Illnesses in Pediatrics: - Classification - Detail Discussion - Diagnosis - Management - PreventionMansoor HasnainNessuna valutazione finora
- 05 Central Nervous SystemDocumento70 pagine05 Central Nervous SystemThetnaungsoeNessuna valutazione finora
- Patient Case Study With H1N1 Influenza VirusDocumento3 paginePatient Case Study With H1N1 Influenza VirusAmera DimatingcalNessuna valutazione finora
- Case Study 1Documento9 pagineCase Study 1andry natanel tonyNessuna valutazione finora
- Case Study LRTIDocumento18 pagineCase Study LRTINorman DyantoNessuna valutazione finora
- COPDCaseStudy NumberThreeDocumento12 pagineCOPDCaseStudy NumberThreeKasturi SekarNessuna valutazione finora
- 01 - Bronchial AsthmaDocumento6 pagine01 - Bronchial AsthmaFrank VaronaNessuna valutazione finora
- Emergency Management of Acute BronchiolitisDocumento26 pagineEmergency Management of Acute BronchiolitisPethuel AgyinNessuna valutazione finora
- Approach To Chronic CoughDocumento31 pagineApproach To Chronic CoughNoreen Ooi Zhi MinNessuna valutazione finora
- Cough - The Challenge of A Targeted Diagnosis: Michael A. Venditto DO, FACOI, FCCPDocumento37 pagineCough - The Challenge of A Targeted Diagnosis: Michael A. Venditto DO, FACOI, FCCPMuhammad Erwin Yamashita100% (1)
- Acute Respiratory InfectionDocumento68 pagineAcute Respiratory InfectionArun GeorgeNessuna valutazione finora
- BronchiolitisDocumento30 pagineBronchiolitisTitusNessuna valutazione finora
- Asthma EmergencyDocumento20 pagineAsthma EmergencyJanice Shaileen KrishnaNessuna valutazione finora
- "Don't Take My Breath Away" A Case Presentation On Pneumocystis PneumoniaDocumento20 pagine"Don't Take My Breath Away" A Case Presentation On Pneumocystis PneumoniaNikki DiocampoNessuna valutazione finora
- Asthma Treatment GuidlineDocumento56 pagineAsthma Treatment GuidlineEsther OdumanyeNessuna valutazione finora
- Case Presentation: Mohammed BarghashDocumento31 pagineCase Presentation: Mohammed BarghashalaaNessuna valutazione finora
- MCC - Copd Roll No 4,37,38,40Documento30 pagineMCC - Copd Roll No 4,37,38,40Anagha M NairNessuna valutazione finora
- Nursing Care Plan For Patient Case 1: Citra Intan Widyasari Nabila Tasya Ayuputri Stephanie Kumala HayatiDocumento22 pagineNursing Care Plan For Patient Case 1: Citra Intan Widyasari Nabila Tasya Ayuputri Stephanie Kumala HayatiALFI NURUL IMANINessuna valutazione finora
- A 2 Years Old Girl Presented With Cyanosis & ClubbingDocumento34 pagineA 2 Years Old Girl Presented With Cyanosis & ClubbingFouzia Zaman ZiniaNessuna valutazione finora
- Asthma in Children My PresentationDocumento49 pagineAsthma in Children My PresentationPutra Skate100% (3)
- CASE PRESENTATION - Chronic Obstructive Pulmonary Disease COPD EmphysemaDocumento25 pagineCASE PRESENTATION - Chronic Obstructive Pulmonary Disease COPD Emphysemaczeremar chanNessuna valutazione finora
- Clerk GCPDocumento19 pagineClerk GCPNikki DiocampoNessuna valutazione finora
- Shortness of Breath: UNC Emergency Medicine Medical Student Lecture SeriesDocumento49 pagineShortness of Breath: UNC Emergency Medicine Medical Student Lecture SeriesGilbert Solomon Tantono100% (1)
- 7 - Respiratory Emergencies and Thoracic Trauma PDFDocumento112 pagine7 - Respiratory Emergencies and Thoracic Trauma PDFRere AngelicaNessuna valutazione finora
- Update Who Aria 2008, SuprihatiDocumento27 pagineUpdate Who Aria 2008, SuprihatiivensNessuna valutazione finora
- Clinical Meet: DR Subas SharmaDocumento79 pagineClinical Meet: DR Subas SharmaSubas SharmaNessuna valutazione finora
- Copd and Asthma FinalDocumento26 pagineCopd and Asthma FinalRainer PoNessuna valutazione finora
- A Case Study On Pediatric Community Acquired Pneumonia-DDocumento58 pagineA Case Study On Pediatric Community Acquired Pneumonia-DAnonymous A5dkn4N3Nessuna valutazione finora
- Understanding Breathlessness in 10'ish Minutes!Documento25 pagineUnderstanding Breathlessness in 10'ish Minutes!ناصر كشلافNessuna valutazione finora
- FIRST NAME, LAST NAME-Mevatia Dhaval Course - 4 GROUP - 463Documento15 pagineFIRST NAME, LAST NAME-Mevatia Dhaval Course - 4 GROUP - 463Mevatia DhavalNessuna valutazione finora
- Cough, Dyspnoea: DR - Veena 2016 - 2017Documento109 pagineCough, Dyspnoea: DR - Veena 2016 - 2017HanisahNessuna valutazione finora
- Case Presentation On Recurrent PULMONARY EMBOLISMDocumento14 pagineCase Presentation On Recurrent PULMONARY EMBOLISMAkas RehmanNessuna valutazione finora
- Welcome RSVDocumento32 pagineWelcome RSVapi-260357356Nessuna valutazione finora
- Nursing Care PlanDocumento2 pagineNursing Care Planusama_salaymehNessuna valutazione finora
- SOPIEDocumento16 pagineSOPIEshing_1987Nessuna valutazione finora
- Information Sheet For CandidatesDocumento7 pagineInformation Sheet For Candidatesfire_n_iceNessuna valutazione finora
- 2016-17 - 1st SemDocumento7 pagine2016-17 - 1st SemMadhura Pushpa kumaraNessuna valutazione finora
- Clinical Pharmacy Asthma: Lecture # 1 by Ms. Fakhsheena AnjumDocumento66 pagineClinical Pharmacy Asthma: Lecture # 1 by Ms. Fakhsheena Anjumgurrya786Nessuna valutazione finora
- Discharge Summary Sample: Rev 11/10 D. Eakin, MDDocumento2 pagineDischarge Summary Sample: Rev 11/10 D. Eakin, MDGem Nicole P. AbrasaldoNessuna valutazione finora
- Mortality Meeting MDocumento11 pagineMortality Meeting MAvian CamelotNessuna valutazione finora
- Case Conference: Pediatric Community Acquired PneumoniaDocumento46 pagineCase Conference: Pediatric Community Acquired PneumoniaElaine Francisse TampusNessuna valutazione finora
- Bronchial Asthma and Acute AsthmaDocumento38 pagineBronchial Asthma and Acute AsthmaFreddy KassimNessuna valutazione finora
- Case PresentationDocumento46 pagineCase PresentationAileen DometitaNessuna valutazione finora
- NCP of Respiratory DistressDocumento3 pagineNCP of Respiratory DistressDarwin QuirimitNessuna valutazione finora
- Diploma in Medical and Health Science Case ClerkingDocumento9 pagineDiploma in Medical and Health Science Case ClerkingWan AmeeramirulzamanNessuna valutazione finora
- Documento de InglesDocumento3 pagineDocumento de InglesEdilsonNessuna valutazione finora
- 2-Shortness of Breath by DR - HananDocumento49 pagine2-Shortness of Breath by DR - HananSoon SheedNessuna valutazione finora
- Acute Exacerbation of COPDDocumento21 pagineAcute Exacerbation of COPDArmaanjeet SinghNessuna valutazione finora
- CopdDocumento20 pagineCopdDhanesh B MNessuna valutazione finora
- Case Studies (CPR)Documento22 pagineCase Studies (CPR)Sadia SundasNessuna valutazione finora
- Gordon WoodDocumento39 pagineGordon WoodjosephNessuna valutazione finora
- Internal Medicine Write Up 1Documento16 pagineInternal Medicine Write Up 1Ariff MahdzubNessuna valutazione finora
- Cleansing in ELBWDocumento22 pagineCleansing in ELBWhana_shamsNessuna valutazione finora
- Paediatric MelioidosisDocumento7 paginePaediatric Melioidosishana_shamsNessuna valutazione finora
- Paediatric MelioidosisDocumento7 paginePaediatric Melioidosishana_shamsNessuna valutazione finora
- Postoperative PyrexiaDocumento24 paginePostoperative Pyrexiahana_shamsNessuna valutazione finora
- CaputDocumento1 paginaCaputhana_shamsNessuna valutazione finora
- Shock in The Pediatric Patient: or Oxygen Don't Go Where The Blood Won't Flow!Documento63 pagineShock in The Pediatric Patient: or Oxygen Don't Go Where The Blood Won't Flow!hana_shamsNessuna valutazione finora
- CPG Management of Venous TromboemlismDocumento63 pagineCPG Management of Venous Tromboemlismapalaginih100% (1)
- محمد سعد طهDocumento3 pagineمحمد سعد طهمحمد سعد طه احمدNessuna valutazione finora
- Paediatrics Ii (A)Documento1 paginaPaediatrics Ii (A)AlolikaNessuna valutazione finora
- Approach To Abdominal PainDocumento4 pagineApproach To Abdominal PainShamen KohNessuna valutazione finora
- Foot DropDocumento2 pagineFoot DropSaravanan SridharanNessuna valutazione finora
- Gastrointestinal Imaging - The Requisites (4e) (2014) (Unitedvrg)Documento435 pagineGastrointestinal Imaging - The Requisites (4e) (2014) (Unitedvrg)crazyballerman80890% (10)
- Hallucinations and Hearing VoicesDocumento4 pagineHallucinations and Hearing VoicesCazacu ParascoviaNessuna valutazione finora
- Case Study About Hypertension With Electrolyte Imbalance Part 3Documento2 pagineCase Study About Hypertension With Electrolyte Imbalance Part 3THE NURSING CORNERS100% (1)
- WCR Annexure - 1 FromDocumento1 paginaWCR Annexure - 1 FromSaikat DawanNessuna valutazione finora
- Dosdos, Bianca Mikaela F. Individual-Activity-Abraham-Aguilas-Case-1Documento4 pagineDosdos, Bianca Mikaela F. Individual-Activity-Abraham-Aguilas-Case-1Bianx Flores DosdosNessuna valutazione finora
- MCQ NelsonDocumento433 pagineMCQ NelsonShashank MisraNessuna valutazione finora
- Primery Survey GadarDocumento11 paginePrimery Survey GadarapryNessuna valutazione finora
- Botulinum ToxinDocumento29 pagineBotulinum Toxinbluecrush1100% (1)
- Respiratory Syncytial Virus in LowerDocumento6 pagineRespiratory Syncytial Virus in LowerShailendra ParajuliNessuna valutazione finora
- Hystrix Like Ichthyosis With DeafnessDocumento3 pagineHystrix Like Ichthyosis With DeafnessjehzamudioNessuna valutazione finora
- Cardiac Auscultation 3696Documento2 pagineCardiac Auscultation 3696nutype01Nessuna valutazione finora
- CBC Reference Value TableDocumento2 pagineCBC Reference Value Tabletommy areanNessuna valutazione finora
- The Aging Voice: Presented by Anastasia Serbalik Presented To Rebecca L. Gould, MSC, CCC-SLPDocumento32 pagineThe Aging Voice: Presented by Anastasia Serbalik Presented To Rebecca L. Gould, MSC, CCC-SLPAtri AmmuluNessuna valutazione finora
- Gastroenteritis:: Nontyphoidal Salmonella InfectionDocumento2 pagineGastroenteritis:: Nontyphoidal Salmonella InfectionYana KostNessuna valutazione finora
- SBP - Tushar Kanti Debnath - 20810066Documento17 pagineSBP - Tushar Kanti Debnath - 20810066PRANJAL KUMARNessuna valutazione finora
- Vector Borne Disease Malaria Dengue Kalazar Chikungunya Filiarisis Indian Council Medical ResearchDocumento44 pagineVector Borne Disease Malaria Dengue Kalazar Chikungunya Filiarisis Indian Council Medical Researchanupsingh775Nessuna valutazione finora
- NCP For UDHDocumento3 pagineNCP For UDHTomohiro HorieNessuna valutazione finora
- The Prevalence and Associated Risk Factors of Musculoskeletal Disorders Among BankersDocumento21 pagineThe Prevalence and Associated Risk Factors of Musculoskeletal Disorders Among BankersNdayambaje EmmanuelNessuna valutazione finora
- Level 10 Quiz V2 - RevisedDocumento4 pagineLevel 10 Quiz V2 - RevisedGordon B.J.Nessuna valutazione finora
- 2012 NCCAOM Herbal Exam QuestionsDocumento10 pagine2012 NCCAOM Herbal Exam QuestionsElizabeth Durkee Neil100% (2)
- Fundamentals of Nursing Practice - MidtermDocumento24 pagineFundamentals of Nursing Practice - MidtermShene Claire VigillaNessuna valutazione finora
- Lung Cancer Translational and Emerging Therapies by Kishan J. PandyaDocumento276 pagineLung Cancer Translational and Emerging Therapies by Kishan J. PandyaADEEL ARSALANNessuna valutazione finora
- Integrated Management On Childhood Illnesses 0101Documento132 pagineIntegrated Management On Childhood Illnesses 0101James Felix Gallano Gales100% (1)
- Rubella Virus: Tatiana Lanzieri, MD Penina Haber, MPH Joseph P. Icenogle, PHD, Ms and Manisha Patel, MD, MsDocumento14 pagineRubella Virus: Tatiana Lanzieri, MD Penina Haber, MPH Joseph P. Icenogle, PHD, Ms and Manisha Patel, MD, Msriska apriliani hendartoNessuna valutazione finora
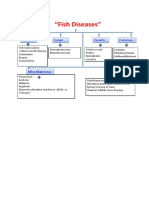
- 202004061939435276sptrivedi Fish DiseasesDocumento19 pagine202004061939435276sptrivedi Fish DiseasesSaravanan arnoldNessuna valutazione finora
- Click To Edit Master Subtitle StyleDocumento41 pagineClick To Edit Master Subtitle StyleMahar NaveedNessuna valutazione finora