Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Spinal cord lesion 2 د.رشاد عبدالغنيDocumento58 pagineSpinal cord lesion 2 د.رشاد عبدالغنيMohammad BelbahaithNessuna valutazione finora
- Epilepsy د.عبدالرحمن سلامDocumento20 pagineEpilepsy د.عبدالرحمن سلامMohammad BelbahaithNessuna valutazione finora
- Spinal cord lesion (Transverse myelitis) د.رشاد عبدالغنيDocumento33 pagineSpinal cord lesion (Transverse myelitis) د.رشاد عبدالغنيMohammad BelbahaithNessuna valutazione finora
- Neuromuscular dis د.رشاد عبدالغنيDocumento47 pagineNeuromuscular dis د.رشاد عبدالغنيMohammad Belbahaith100% (1)
- Motor neurone disease د.رشاد عبدالغنيDocumento18 pagineMotor neurone disease د.رشاد عبدالغنيMohammad BelbahaithNessuna valutazione finora
- Urinary Tract Infections د.أحمد الأهنوميDocumento44 pagineUrinary Tract Infections د.أحمد الأهنوميMohammad BelbahaithNessuna valutazione finora
- Nurological Emergencies د.عارفDocumento54 pagineNurological Emergencies د.عارفMohammad BelbahaithNessuna valutazione finora
- Breast د.رامز الأسوديDocumento15 pagineBreast د.رامز الأسوديMohammad BelbahaithNessuna valutazione finora
- Investigation of CNS د.محمد سلامDocumento42 pagineInvestigation of CNS د.محمد سلامMohammad BelbahaithNessuna valutazione finora
- Gestational Trophoblastic Disease (GTD)Documento72 pagineGestational Trophoblastic Disease (GTD)Mohammad BelbahaithNessuna valutazione finora
- Bladder TumorsDocumento36 pagineBladder TumorsMohammad BelbahaithNessuna valutazione finora
- Neurological symptoms د.محمد سلامDocumento20 pagineNeurological symptoms د.محمد سلامMohammad BelbahaithNessuna valutazione finora
- Thromboembolic Disease in Pregnancy د.علية شعيبDocumento50 pagineThromboembolic Disease in Pregnancy د.علية شعيبMohammad Belbahaith0% (1)
- Preterm labour د.علية شعيبDocumento58 paginePreterm labour د.علية شعيبMohammad BelbahaithNessuna valutazione finora
- Ultrasound in 1st, 2nd & 3rd trimester د.رامز الأسوديDocumento13 pagineUltrasound in 1st, 2nd & 3rd trimester د.رامز الأسوديMohammad BelbahaithNessuna valutazione finora
- Art 16-18Documento528 pagineArt 16-18ErudíhenNessuna valutazione finora
- 7UM512 CatalogueDocumento12 pagine7UM512 Cataloguebuianhtuan1980Nessuna valutazione finora
- E2870-13 Standard Test Method For Evaluating RelativDocumento6 pagineE2870-13 Standard Test Method For Evaluating RelativA MusaverNessuna valutazione finora
- Transcendental Meditation (Four Lectures by Silo)Documento49 pagineTranscendental Meditation (Four Lectures by Silo)nmjoshi77859100% (2)
- Ford6000cd Rear ConnectorDocumento2 pagineFord6000cd Rear ConnectorAnonymous WcYW9AeNessuna valutazione finora
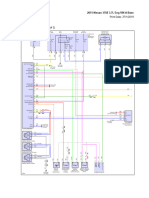
- 2015 Nissan 370Z 3.7L Eng VIN A BaseDocumento69 pagine2015 Nissan 370Z 3.7L Eng VIN A BaseData TécnicaNessuna valutazione finora
- Action Plan Gulayan Sa PaaralanDocumento2 pagineAction Plan Gulayan Sa PaaralanAntonio ArienzaNessuna valutazione finora
- Semicounductors & Pn-Junction (Complete)Documento47 pagineSemicounductors & Pn-Junction (Complete)Khalid AliNessuna valutazione finora
- Inventory of Flood Bund PunjabDocumento26 pagineInventory of Flood Bund PunjabguildkeyNessuna valutazione finora
- Compaction - AsphaltDocumento32 pagineCompaction - Asphaltrskcad100% (1)
- Power System Analysis and Design EE-461: Tassawar Kazmi Lecturer, EE Department, Seecs, NustDocumento10 paginePower System Analysis and Design EE-461: Tassawar Kazmi Lecturer, EE Department, Seecs, NustShahab SaqibNessuna valutazione finora
- Tycho BraheDocumento3 pagineTycho BraheAienna Lacaya MatabalanNessuna valutazione finora
- 3rd Quarter Performance TaskDocumento3 pagine3rd Quarter Performance TaskJaime CrispinoNessuna valutazione finora
- Hipertensiunea Arteriala - Cauze Si TratamenteDocumento25 pagineHipertensiunea Arteriala - Cauze Si TratamenteClaudia MurguNessuna valutazione finora
- ASTM E 1066 - 95 Standard Practice For Ammonia Colorimetric Leak Testing PDFDocumento5 pagineASTM E 1066 - 95 Standard Practice For Ammonia Colorimetric Leak Testing PDFАртем ТитовNessuna valutazione finora
- Sales Training Deck Updated July 2022Documento40 pagineSales Training Deck Updated July 2022Thanh MinhNessuna valutazione finora
- Simple Euler StrutDocumento16 pagineSimple Euler StrutDaniel MabengoNessuna valutazione finora
- Harrington SOAP NoteDocumento5 pagineHarrington SOAP NoteDanielle100% (4)
- 03N - Top Level View of Computer Function and InterconnectionDocumento38 pagine03N - Top Level View of Computer Function and InterconnectionDoc TelNessuna valutazione finora
- Sawla - Laska (Lot - I) Road Project Hydrology - Hydraulics MDocumento64 pagineSawla - Laska (Lot - I) Road Project Hydrology - Hydraulics Mashe zinab100% (2)
- Water Treatment Lecture 4Documento34 pagineWater Treatment Lecture 4pramudita nadiahNessuna valutazione finora
- Maxon - Gas Electro-Mechanical ValvesDocumento4 pagineMaxon - Gas Electro-Mechanical ValvesThiagoNessuna valutazione finora
- Kim, KDM, Sim, SDM PDFDocumento12 pagineKim, KDM, Sim, SDM PDFKavan Gt12Nessuna valutazione finora
- Mikrotik Kung Fu Kitab 2Documento68 pagineMikrotik Kung Fu Kitab 2aditya ferdiansyahNessuna valutazione finora
- Essenza Refurbished Siemens MRI MachineDocumento2 pagineEssenza Refurbished Siemens MRI Machinetech.arnicahealthNessuna valutazione finora
- BookDocumento28 pagineBookFebrian Wardoyo100% (1)
- Darmoatmodjo 2023Documento7 pagineDarmoatmodjo 2023mayaNessuna valutazione finora
- FEED Deliverable List (Sample) : Project InformationDocumento3 pagineFEED Deliverable List (Sample) : Project Informationamilasri100% (1)
- DE (Diatomaceous Earth) BenefitsDocumento9 pagineDE (Diatomaceous Earth) BenefitsIlqa116100% (1)
- 1-Theory of Metal Cutting PDFDocumento144 pagine1-Theory of Metal Cutting PDFNithinArvindNessuna valutazione finora