Potrebbero piacerti anche
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Cardiac MurmursDocumento3 pagineCardiac MurmursDanielleNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- DiltiazemDocumento2 pagineDiltiazemE100% (1)
- Common - CardioDocumento91 pagineCommon - CardioHanadi UmhanayNessuna valutazione finora
- Cardiac Physical ExamDocumento45 pagineCardiac Physical ExamARIANNE JOY TAMARAY100% (1)
- Cardiomyopathy: Mrs. D. Melba Sahaya Sweety M.SC Nursing GimsarDocumento55 pagineCardiomyopathy: Mrs. D. Melba Sahaya Sweety M.SC Nursing GimsarD. Melba S.S ChinnaNessuna valutazione finora
- Heart Disease in PregnancyDocumento20 pagineHeart Disease in PregnancyAnironOrionNessuna valutazione finora
- Aortic StenosisDocumento11 pagineAortic StenosisIra Anuddin100% (1)
- Rheumatic Heart DiseaseDocumento43 pagineRheumatic Heart DiseaseVickeeNessuna valutazione finora
- ECG Red BookDocumento54 pagineECG Red BookHilbertHeungNessuna valutazione finora
- PALS Nitty Gritty Study Guide FINALDocumento11 paginePALS Nitty Gritty Study Guide FINALuncmikee1997100% (1)
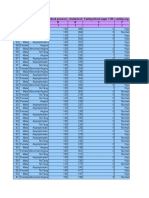
- Age Sex Chest Pain Type Blood Pressure Cholesterol Fasting Blood Sugar 120 Resting Ecg R C C R R C C I I I I I I IDocumento14 pagineAge Sex Chest Pain Type Blood Pressure Cholesterol Fasting Blood Sugar 120 Resting Ecg R C C R R C C I I I I I I Isantu4_1111Nessuna valutazione finora
- Clinical Audit On Code BlueDocumento7 pagineClinical Audit On Code BlueSunny AnthonyNessuna valutazione finora
- CCHD Screening - MohDocumento6 pagineCCHD Screening - MohAhmed Mohammed100% (1)
- Cardiology - MRCP NotesDocumento5 pagineCardiology - MRCP NotesShazina Kohli100% (1)
- Clinical ECG RoundsDocumento2 pagineClinical ECG RoundsKai Siang ChanNessuna valutazione finora
- The ElectrocardiogramDocumento53 pagineThe ElectrocardiogramJEM93Nessuna valutazione finora
- Multiple and Mixed Valvular Heart DiseaseDocumento13 pagineMultiple and Mixed Valvular Heart DiseaseВенцислав МирчевNessuna valutazione finora
- FREE 2021 ACLS Study Guide - ACLS Made Easy!Documento32 pagineFREE 2021 ACLS Study Guide - ACLS Made Easy!Alen ArguellesNessuna valutazione finora
- ECG NotesDocumento8 pagineECG NotesPeer TutorNessuna valutazione finora
- Palpitations: DR Polamuri Tabitha PG First YrDocumento37 paginePalpitations: DR Polamuri Tabitha PG First YrNinaNessuna valutazione finora
- Ecg For AnkiDocumento3 pagineEcg For AnkijNessuna valutazione finora
- Calcium Channel BlockersDocumento2 pagineCalcium Channel BlockersBrittany RamirezNessuna valutazione finora
- Tricuspid Valve DiseaseDocumento20 pagineTricuspid Valve Diseasesarguss14100% (1)
- The ECG in Hypothermia - Osborn WavesDocumento2 pagineThe ECG in Hypothermia - Osborn WavesVid MirosevicNessuna valutazione finora
- Tutorial Antianginal DrugsDocumento2 pagineTutorial Antianginal DrugsAbdul MosheenNessuna valutazione finora
- 5 Step EKG InterpretationDocumento1 pagina5 Step EKG InterpretationSibel ErtuğrulNessuna valutazione finora
- Cardiac Implantable Electronic DevicesDocumento49 pagineCardiac Implantable Electronic DevicespriyathasanNessuna valutazione finora
- Nuclear CaseDocumento106 pagineNuclear CaseAkramNessuna valutazione finora
- 7.article - Nurse Method For Quick Interpret ECGDocumento13 pagine7.article - Nurse Method For Quick Interpret ECGEvieta CallysthaNessuna valutazione finora
- @brainandheart20 @brainandheart20 Brain and Heart 2020Documento7 pagine@brainandheart20 @brainandheart20 Brain and Heart 2020Mukhlisin RizalNessuna valutazione finora