Potrebbero piacerti anche
- Improving Revenue and Profitability: IFC, International Private Healthcare Conference, 2009Documento25 pagineImproving Revenue and Profitability: IFC, International Private Healthcare Conference, 2009Jyotika GuptaNessuna valutazione finora
- Indian Healthcare Business ModelsDocumento27 pagineIndian Healthcare Business ModelsMahesh MahtoliaNessuna valutazione finora
- Medtronic MITG Investor Day PresentationDocumento22 pagineMedtronic MITG Investor Day PresentationmedtechyNessuna valutazione finora
- Mayo Clinic Marketing ResearchDocumento14 pagineMayo Clinic Marketing Researchshivam joshiNessuna valutazione finora
- Mediclaim Insurance: - M.ANUSHA (10AD03) - PREETHI (10AD22) - Poorna Chandra (10ad40)Documento22 pagineMediclaim Insurance: - M.ANUSHA (10AD03) - PREETHI (10AD22) - Poorna Chandra (10ad40)Preethi LathicaNessuna valutazione finora
- Future Trends in Insurance - Trevor RorbyeDocumento23 pagineFuture Trends in Insurance - Trevor Rorbyekwtam338Nessuna valutazione finora
- C Mmittees B Senior Issues 2012 Fall NM LTC Hearing Presentations Cohen RevisedDocumento25 pagineC Mmittees B Senior Issues 2012 Fall NM LTC Hearing Presentations Cohen RevisedswotavatorNessuna valutazione finora
- Mayo ClinicDocumento8 pagineMayo ClinicTomás RodriguesNessuna valutazione finora
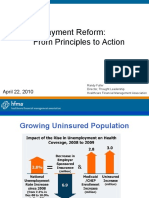
- Payment Reform: From Principles to ActionDocumento34 paginePayment Reform: From Principles to Actionibson045001256Nessuna valutazione finora
- The Affordable Care ActDocumento40 pagineThe Affordable Care ActGurvinder SinghNessuna valutazione finora
- Group 6 Assignment 3: Quickmedx Inc. - Case AnalysisDocumento15 pagineGroup 6 Assignment 3: Quickmedx Inc. - Case Analysisbalu230180% (5)
- Religare Report - FormattedDocumento55 pagineReligare Report - FormattedAbhijit RoyNessuna valutazione finora
- Financial Resilience Newsletter Issue 6 - July 2019Documento5 pagineFinancial Resilience Newsletter Issue 6 - July 2019Max EvansNessuna valutazione finora
- Medical Devices Supply Chain OptimizationDocumento12 pagineMedical Devices Supply Chain OptimizationAbhishek Sharma100% (1)
- Using Innovation To Increase AccessibilityDocumento36 pagineUsing Innovation To Increase AccessibilitySatrasala AshokkumarNessuna valutazione finora
- Parallel 12 Breaking The Insurance MouldDocumento46 pagineParallel 12 Breaking The Insurance MouldnvtcmnNessuna valutazione finora
- Six Sigma and Its Application To HealthcareDocumento20 pagineSix Sigma and Its Application To HealthcareAkash Bhagat100% (1)
- Healthcare Sector Analysis: Prepared by Ariel Imas Robert Candella Nanda WinDocumento38 pagineHealthcare Sector Analysis: Prepared by Ariel Imas Robert Candella Nanda WinAnbu RajNessuna valutazione finora
- Using the Balanced Scorecard to Drive Strategic ChangeDocumento30 pagineUsing the Balanced Scorecard to Drive Strategic ChangeSonya DewiNessuna valutazione finora
- Levac - Immunization From LeprosyDocumento26 pagineLevac - Immunization From LeprosyVarun GuptaNessuna valutazione finora
- CORPORATE OVERVIEW IN HEALTHCAREDocumento20 pagineCORPORATE OVERVIEW IN HEALTHCAREKrishanth PptNessuna valutazione finora
- Medtech in Asia Committing at Scale To Raise Standards of Care For Patients PDFDocumento49 pagineMedtech in Asia Committing at Scale To Raise Standards of Care For Patients PDFKunalNessuna valutazione finora
- Presentation On Business Plan: SmartDocumento22 paginePresentation On Business Plan: SmartManishNessuna valutazione finora
- Business Plan For LaboratoryDocumento22 pagineBusiness Plan For LaboratoryManish Rastogi100% (3)
- Presented by AlhassanDocumento12 paginePresented by AlhassanGabriel Alva AnkrahNessuna valutazione finora
- Ndis Costs OverviewDocumento69 pagineNdis Costs OverviewAkshay KumarNessuna valutazione finora
- Scripps Health Section 3Documento8 pagineScripps Health Section 3DanyNessuna valutazione finora
- Centric HealthDocumento38 pagineCentric HealthJenny QuachNessuna valutazione finora
- Herrmann Et Al. - 2018 - Digital Transformation and Disruption of The HealtDocumento8 pagineHerrmann Et Al. - 2018 - Digital Transformation and Disruption of The HealtRosliana MahardhikaNessuna valutazione finora
- Case 2Documento17 pagineCase 2Suraj KumarNessuna valutazione finora
- The Future of The Financial System and The Money and Capital MarketsDocumento28 pagineThe Future of The Financial System and The Money and Capital MarketsBSA3Tagum MariletNessuna valutazione finora
- Supply Chain Guide by Quasar-MedDocumento25 pagineSupply Chain Guide by Quasar-MedDiniy YusofNessuna valutazione finora
- Pahal Healthcare Innovation Report Print Ready 14th MayDocumento40 paginePahal Healthcare Innovation Report Print Ready 14th MayAmar SharmaNessuna valutazione finora
- Digilog BrochureDocumento8 pagineDigilog BrochureMark AldissNessuna valutazione finora
- Faster, Better, Cheaper: Creating Opportunities in A Converging Healthcare IndustryDocumento10 pagineFaster, Better, Cheaper: Creating Opportunities in A Converging Healthcare IndustryAnkit SrivastavaNessuna valutazione finora
- LO 3 - Chapter 7 Healthcare BenefitsDocumento24 pagineLO 3 - Chapter 7 Healthcare BenefitssalwaNessuna valutazione finora
- Project Title: Strategic Marketing Plan For Project Details: Hub and Spoke Model of Healthcare Services in Kasaragod Market & CompetitorsDocumento21 pagineProject Title: Strategic Marketing Plan For Project Details: Hub and Spoke Model of Healthcare Services in Kasaragod Market & CompetitorsAgri Finance KnowledgeNessuna valutazione finora
- A-Consulting Case - Group 10 FinalDocumento12 pagineA-Consulting Case - Group 10 FinalMayur Dadia100% (1)
- LEADS Brochure - Final Published VersionDocumento4 pagineLEADS Brochure - Final Published VersionChevronelleNessuna valutazione finora
- Excellence in Diagnostic CareDocumento20 pagineExcellence in Diagnostic CareDominic LiangNessuna valutazione finora
- Assignent 2 - SDMMDocumento16 pagineAssignent 2 - SDMMwipbanuaNessuna valutazione finora
- Lexicon ProfileDocumento15 pagineLexicon ProfileMeenu Grover SharmaNessuna valutazione finora
- Reliance Life InsuranceDocumento19 pagineReliance Life InsurancesakshichitkaraNessuna valutazione finora
- Business CommunicationDocumento15 pagineBusiness Communicationmaleeha shahzadNessuna valutazione finora
- FoodSafety Brochure Ukraine EngDocumento12 pagineFoodSafety Brochure Ukraine EngIzudin OkicNessuna valutazione finora
- 758o 2 PDFDocumento374 pagine758o 2 PDFAmr A. MohamedNessuna valutazione finora
- Healthcare Domain TrainingDocumento19 pagineHealthcare Domain TrainingShashank Raj50% (2)
- AHM 250 SummaryDocumento117 pagineAHM 250 Summarysenthilj82Nessuna valutazione finora
- GROWTH OF GLOBAL SUPPLY CHAINDocumento15 pagineGROWTH OF GLOBAL SUPPLY CHAINAncyNessuna valutazione finora
- J&J Quest Isb CynosureDocumento7 pagineJ&J Quest Isb CynosureHimanshu BhatiaNessuna valutazione finora
- India Power Sector: Challenges & Investment OpportunitiesDocumento23 pagineIndia Power Sector: Challenges & Investment OpportunitiesYasir HamidNessuna valutazione finora
- AHM 250 SummaryDocumento116 pagineAHM 250 SummaryDinesh Anbumani100% (5)
- Diagnostic Services IndiaDocumento1 paginaDiagnostic Services IndianikeshlambaNessuna valutazione finora
- IBM IIW OverviewDocumento36 pagineIBM IIW Overviewd_sengNessuna valutazione finora
- Supply Chain ManagementDocumento22 pagineSupply Chain ManagementPayal Nayak100% (1)
- Case 2 Compress PDFDocumento17 pagineCase 2 Compress PDFAbhinav KumarNessuna valutazione finora
- Textbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersDa EverandTextbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersNessuna valutazione finora
- How to Grow When Markets Don't (Review and Analysis of Slywotzky and Wise's Book)Da EverandHow to Grow When Markets Don't (Review and Analysis of Slywotzky and Wise's Book)Nessuna valutazione finora
- Using ISO 9001 in Healthcare: Applications for Quality Systems, Performance Improvement, Clinical Integration, and AccreditationDa EverandUsing ISO 9001 in Healthcare: Applications for Quality Systems, Performance Improvement, Clinical Integration, and AccreditationNessuna valutazione finora
- The Art of the Heal: A Health Executive’s Guide to Innovating HospitalsDa EverandThe Art of the Heal: A Health Executive’s Guide to Innovating HospitalsNessuna valutazione finora
- Case5 Can CrusherDocumento6 pagineCase5 Can CrusherBalthasar Sebastian LumbanTobingNessuna valutazione finora
- A Joint VentureDocumento4 pagineA Joint Venturesadaf mustafaNessuna valutazione finora
- Equity Research AssignmentDocumento3 pagineEquity Research Assignment201812099 imtnagNessuna valutazione finora
- Castorama 3DDocumento4 pagineCastorama 3Dmarc johanNessuna valutazione finora
- Lecture Notes in Inventory ManagementDocumento50 pagineLecture Notes in Inventory ManagementBruno Saturn100% (1)
- Test Bank - Chapter 16Documento25 pagineTest Bank - Chapter 16Jihad NakibNessuna valutazione finora
- Corporate Failure (Assignment)Documento9 pagineCorporate Failure (Assignment)Talha MunirNessuna valutazione finora
- Proposed DividebdDocumento34 pagineProposed DividebdPiyush SrivastavaNessuna valutazione finora
- Introduction to Financial Accounting Chapter on DepreciationDocumento61 pagineIntroduction to Financial Accounting Chapter on DepreciationAlty StelleNessuna valutazione finora
- Engineering Economics and Management B.E. 3 /4 Semester: Gujarat Technological UniversityDocumento2 pagineEngineering Economics and Management B.E. 3 /4 Semester: Gujarat Technological UniversityShital Solanki MakwanaNessuna valutazione finora
- Project Report: "Transfer Pricing"Documento34 pagineProject Report: "Transfer Pricing"Dev RaiNessuna valutazione finora
- Demand For Milk Grows in IndiaDocumento7 pagineDemand For Milk Grows in IndiaUtsav DubeyNessuna valutazione finora
- Multiple Choice: - ConceptualDocumento11 pagineMultiple Choice: - Conceptualjustinng191Nessuna valutazione finora
- IBPS CLERK MAINS 2018 Memory Based Quant SOL PDFDocumento13 pagineIBPS CLERK MAINS 2018 Memory Based Quant SOL PDFAishwarya Devkar PatilNessuna valutazione finora
- Lecture 1: Introduction to International Financial ManagementDocumento17 pagineLecture 1: Introduction to International Financial ManagementMahbubul Islam KoushickNessuna valutazione finora
- Summer Training Report - RitikaDocumento69 pagineSummer Training Report - Ritikaritika_honey2377% (30)
- 2 Production: Cbi Market Survey: The Stationery, Office and School Supplies Market in The EuDocumento4 pagine2 Production: Cbi Market Survey: The Stationery, Office and School Supplies Market in The Euthomas_joseph_18Nessuna valutazione finora
- Krugman SolMan CH04Documento16 pagineKrugman SolMan CH04Edson SarmientoNessuna valutazione finora
- Assignment DFA6127Documento3 pagineAssignment DFA6127parwez_0505Nessuna valutazione finora
- Agency Callable Primer 07mar07Documento18 pagineAgency Callable Primer 07mar07Neil SchofieldNessuna valutazione finora
- Time Value of Money - Part1Documento28 pagineTime Value of Money - Part1Alex JavierNessuna valutazione finora
- Is - 7337-2010-Project Management - Glossary of TermsDocumento12 pagineIs - 7337-2010-Project Management - Glossary of TermsPinjala Yagna Kumar DevangaNessuna valutazione finora
- Understanding Financial Statements: Student - Feedback@sti - EduDocumento6 pagineUnderstanding Financial Statements: Student - Feedback@sti - Eduvince mendozaNessuna valutazione finora
- Factor Affecting Rural MarketingDocumento5 pagineFactor Affecting Rural Marketingshaileshkumargupta100% (1)
- Gitman Chapter 14 Divident PolicyDocumento59 pagineGitman Chapter 14 Divident PolicyArif SharifNessuna valutazione finora
- mkt421 FINALDocumento25 paginemkt421 FINALherezulfadhliNessuna valutazione finora
- M2 L4 Basic MicroeconomicsDocumento21 pagineM2 L4 Basic MicroeconomicsBERNARD CALZARNessuna valutazione finora
- Chelsea Parker 2442series HY25-2142-M1Documento20 pagineChelsea Parker 2442series HY25-2142-M1Carlos Alberto Ramirez ParraNessuna valutazione finora
- Customer SatisfactionDocumento17 pagineCustomer Satisfactionrcindia1Nessuna valutazione finora
- ICSI - ESOP Presentation-G SharmaDocumento41 pagineICSI - ESOP Presentation-G SharmaK.S.V.N.S.KAMESWARA RAO100% (3)