Potrebbero piacerti anche
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Case Presentation ParaplegiaDocumento51 pagineCase Presentation ParaplegiaHussain Azhar100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Dr. Adeel Ahmed Waheed: House Officer M-4Documento84 pagineDr. Adeel Ahmed Waheed: House Officer M-4Hussain AzharNessuna valutazione finora
- Conceptual Data Modeling and Database Design Volume 1 - The Shortest Advisable Path A Fully Algorithmic ApproachDocumento662 pagineConceptual Data Modeling and Database Design Volume 1 - The Shortest Advisable Path A Fully Algorithmic ApproachErkan50% (2)
- Heat Combustion Laboratory ReportDocumento8 pagineHeat Combustion Laboratory ReportSteven Lee100% (1)
- Cics Class 05Documento18 pagineCics Class 05HarithaNessuna valutazione finora
- Mathematics Class 10 CBSE (NCERT)Documento369 pagineMathematics Class 10 CBSE (NCERT)LinoNessuna valutazione finora
- Approach To Unconsious PTDocumento62 pagineApproach To Unconsious PTHussain AzharNessuna valutazione finora
- Self-Coached Climber - The Guide To Movem - Dan M (1) HagueDocumento376 pagineSelf-Coached Climber - The Guide To Movem - Dan M (1) HagueBill Frisch100% (1)
- Anam FinalDocumento82 pagineAnam FinalHussain AzharNessuna valutazione finora
- Ion SyndromeDocumento67 pagineIon SyndromeHussain AzharNessuna valutazione finora
- DVT - 2 FaizaDocumento65 pagineDVT - 2 FaizaHussain AzharNessuna valutazione finora
- DKA Concepts and ManagementDocumento22 pagineDKA Concepts and ManagementMohammad AliNessuna valutazione finora
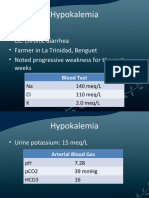
- HypokalemiaDocumento12 pagineHypokalemiaMohammad AliNessuna valutazione finora
- Dka 31-05-11Documento52 pagineDka 31-05-11Hussain AzharNessuna valutazione finora
- Electrolyte Disturbaces - Hyponatremia and HypernatremiaDocumento41 pagineElectrolyte Disturbaces - Hyponatremia and HypernatremiaMohammad AliNessuna valutazione finora
- Liver Function Test FinalDocumento98 pagineLiver Function Test FinalHussain AzharNessuna valutazione finora
- Enteric FeverDocumento63 pagineEnteric FeverHussain AzharNessuna valutazione finora
- EFFA PRESENTATNhepatic EncephalopathyDocumento50 pagineEFFA PRESENTATNhepatic EncephalopathyHussain AzharNessuna valutazione finora
- DVT&PE Final 1Documento59 pagineDVT&PE Final 1Hussain AzharNessuna valutazione finora
- DVTDocumento32 pagineDVTHussain AzharNessuna valutazione finora
- CP Najma 97Documento75 pagineCP Najma 97Hussain AzharNessuna valutazione finora
- Dengue 2009Documento53 pagineDengue 2009Hussain AzharNessuna valutazione finora
- Case Presentation 2Documento53 pagineCase Presentation 2Hussain AzharNessuna valutazione finora
- Case Presentation Hypokalemic ManDocumento61 pagineCase Presentation Hypokalemic ManHussain AzharNessuna valutazione finora
- Copd Final 97-2003hiraaDocumento41 pagineCopd Final 97-2003hiraaHussain AzharNessuna valutazione finora
- Asthma: Presentation By: Dr. Zunaira Nawaz Dr. Nida ShafiqueDocumento47 pagineAsthma: Presentation By: Dr. Zunaira Nawaz Dr. Nida ShafiqueMohammad AliNessuna valutazione finora
- AKIDocumento83 pagineAKIHussain AzharNessuna valutazione finora
- AntibioticsDocumento49 pagineAntibioticsHussain AzharNessuna valutazione finora
- Acute Renal FailureDocumento120 pagineAcute Renal FailureHussain AzharNessuna valutazione finora
- AnemiaDocumento37 pagineAnemiaHussain AzharNessuna valutazione finora
- ABG S Final and Last TouchDocumento88 pagineABG S Final and Last TouchHussain AzharNessuna valutazione finora
- An Approach To Anemic PatientDocumento79 pagineAn Approach To Anemic PatientHussain AzharNessuna valutazione finora
- Acute Exacerbation of COPDDocumento14 pagineAcute Exacerbation of COPDMohammad AliNessuna valutazione finora
- Acrf CDocumento70 pagineAcrf CHussain AzharNessuna valutazione finora
- OptQuest User ManualDocumento190 pagineOptQuest User ManualYamal E Askoul TNessuna valutazione finora
- A Conjunction Is The Glue That Holds WordsDocumento2 pagineA Conjunction Is The Glue That Holds WordsYamson MillerJrNessuna valutazione finora
- Catalogo Carbones Helwig GDE-006Documento17 pagineCatalogo Carbones Helwig GDE-006Sergio HernandezNessuna valutazione finora
- Essential Statistics For The Behavioral Sciences 1st Edition Privitera Solutions ManualDocumento7 pagineEssential Statistics For The Behavioral Sciences 1st Edition Privitera Solutions Manualspinifexcandock8zf100% (26)
- Podar International School Chinchwad STD Xi - (I Unit Test) Subject: Computer Science Date: 8-9-2020 Marks: 40Documento3 paginePodar International School Chinchwad STD Xi - (I Unit Test) Subject: Computer Science Date: 8-9-2020 Marks: 40Shriniwas KulkarniNessuna valutazione finora
- Welding Machine CatalogueDocumento12 pagineWelding Machine CatalogueRodney LanagNessuna valutazione finora
- 12.6 Perform An Activity - Measuring The Critical Angle For Various MediaDocumento2 pagine12.6 Perform An Activity - Measuring The Critical Angle For Various MediaRajeshri SoniNessuna valutazione finora
- DCT Dual Clutch TransmissionDocumento16 pagineDCT Dual Clutch TransmissionSudharshan SrinathNessuna valutazione finora
- Correct AnswerDocumento120 pagineCorrect Answerdebaprasad ghosh100% (1)
- Forrester Roi StudyDocumento30 pagineForrester Roi StudymcgettsNessuna valutazione finora
- p-4500 Technical InformationDocumento13 paginep-4500 Technical InformationElhoiNessuna valutazione finora
- Final Project Regenerative BrakingDocumento6 pagineFinal Project Regenerative Brakingdims irifiyinNessuna valutazione finora
- ALE Between Two SAP SystemsDocumento24 pagineALE Between Two SAP Systemsraghava nimmala100% (1)
- Math10 Week3Day4 Polynomial-EqnsDocumento44 pagineMath10 Week3Day4 Polynomial-EqnsMark Cañete PunongbayanNessuna valutazione finora
- Etap Help PDFDocumento2 pagineEtap Help PDFRebeccaNessuna valutazione finora
- 3-Lecture 03 Translational Mechanical System3-SDocumento23 pagine3-Lecture 03 Translational Mechanical System3-SHamza KhanNessuna valutazione finora
- Applications and Interpretation Standard SpecimensDocumento56 pagineApplications and Interpretation Standard SpecimensNahir ClaraNessuna valutazione finora
- BMW M5 ConfigurationDocumento12 pagineBMW M5 ConfigurationprasadNessuna valutazione finora
- Inductive Proximity Sensors: Brett Anderson ECE 5230 Assignment #1Documento27 pagineInductive Proximity Sensors: Brett Anderson ECE 5230 Assignment #1Rodz Gier JrNessuna valutazione finora
- Effect of Temperature on Chemical ReactionDocumento8 pagineEffect of Temperature on Chemical ReactionnajihahNessuna valutazione finora
- MCB and ELCB PDFDocumento35 pagineMCB and ELCB PDFChris AntoniouNessuna valutazione finora
- PSD60-2R: Operation ManualDocumento22 paginePSD60-2R: Operation ManualOscar SantanaNessuna valutazione finora
- Ductile deformation finite strain analysisDocumento27 pagineDuctile deformation finite strain analysisJorgeBarriosMurielNessuna valutazione finora
- Digital and Analog SignalsDocumento10 pagineDigital and Analog SignalsSrishti GargNessuna valutazione finora
- Unit - L: List and Explain The Functions of Various Parts of Computer Hardware and SoftwareDocumento50 pagineUnit - L: List and Explain The Functions of Various Parts of Computer Hardware and SoftwareMallapuram Sneha RaoNessuna valutazione finora