Potrebbero piacerti anche
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- High Yield Internal Medicine Compatible VersionDocumento100 pagineHigh Yield Internal Medicine Compatible VersionAhsan X Baig100% (5)
- Acute MedicineDocumento321 pagineAcute MedicineMontasir Ahmed100% (18)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Dr. Adeel Ahmed Waheed: House Officer M-4Documento84 pagineDr. Adeel Ahmed Waheed: House Officer M-4Hussain AzharNessuna valutazione finora
- Pulmonaryembolism 150329161109 Conversion Gate01Documento60 paginePulmonaryembolism 150329161109 Conversion Gate01Rafika RaraNessuna valutazione finora
- Pulmonology Step2 CKDocumento22 paginePulmonology Step2 CKsarwat86% (7)
- TestBank Lewis Medical Surgical Nursing 11th 2020.pdf-282-305Documento24 pagineTestBank Lewis Medical Surgical Nursing 11th 2020.pdf-282-305هدوء النسمةNessuna valutazione finora
- Pulmonary EmbolismDocumento4 paginePulmonary Embolismemmag1221100% (1)
- Guide To Clerking 2014Documento24 pagineGuide To Clerking 2014Ridhwan Amid100% (1)
- Pulmonary EmbolismDocumento28 paginePulmonary EmbolismMohamedEzzNessuna valutazione finora
- NCM 118 - Lesson 3 (Pulmonary Embolism)Documento4 pagineNCM 118 - Lesson 3 (Pulmonary Embolism)Bobby Christian DuronNessuna valutazione finora
- Approach To Unconsious PTDocumento62 pagineApproach To Unconsious PTHussain AzharNessuna valutazione finora
- Case Presentation ParaplegiaDocumento51 pagineCase Presentation ParaplegiaHussain Azhar100% (2)
- Mksap PulmonaryDocumento77 pagineMksap PulmonaryAna Roman100% (4)
- K HomeosDocumento47 pagineK HomeosHussain AzharNessuna valutazione finora
- EFFA PRESENTATNhepatic EncephalopathyDocumento50 pagineEFFA PRESENTATNhepatic EncephalopathyHussain AzharNessuna valutazione finora
- Ion SyndromeDocumento67 pagineIon SyndromeHussain AzharNessuna valutazione finora
- Anam FinalDocumento82 pagineAnam FinalHussain AzharNessuna valutazione finora
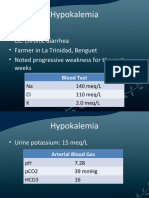
- HypokalemiaDocumento12 pagineHypokalemiaMohammad AliNessuna valutazione finora
- Liver Function Test FinalDocumento98 pagineLiver Function Test FinalHussain AzharNessuna valutazione finora
- Electrolyte Disturbaces - Hyponatremia and HypernatremiaDocumento41 pagineElectrolyte Disturbaces - Hyponatremia and HypernatremiaMohammad AliNessuna valutazione finora
- DVT - 2 FaizaDocumento65 pagineDVT - 2 FaizaHussain AzharNessuna valutazione finora
- Enteric FeverDocumento63 pagineEnteric FeverHussain AzharNessuna valutazione finora
- DKA Concepts and ManagementDocumento22 pagineDKA Concepts and ManagementMohammad AliNessuna valutazione finora
- Dengue 2009Documento53 pagineDengue 2009Hussain AzharNessuna valutazione finora
- Asthma: Presentation By: Dr. Zunaira Nawaz Dr. Nida ShafiqueDocumento47 pagineAsthma: Presentation By: Dr. Zunaira Nawaz Dr. Nida ShafiqueMohammad AliNessuna valutazione finora
- Dka 31-05-11Documento52 pagineDka 31-05-11Hussain AzharNessuna valutazione finora
- Copd Final 97-2003hiraaDocumento41 pagineCopd Final 97-2003hiraaHussain AzharNessuna valutazione finora
- Case Presentation 2Documento53 pagineCase Presentation 2Hussain AzharNessuna valutazione finora
- DVTDocumento32 pagineDVTHussain AzharNessuna valutazione finora
- CP Najma 97Documento75 pagineCP Najma 97Hussain AzharNessuna valutazione finora
- Case Presentation Hypokalemic ManDocumento61 pagineCase Presentation Hypokalemic ManHussain AzharNessuna valutazione finora
- AnemiaDocumento37 pagineAnemiaHussain AzharNessuna valutazione finora
- AntibioticsDocumento49 pagineAntibioticsHussain AzharNessuna valutazione finora
- AKIDocumento83 pagineAKIHussain AzharNessuna valutazione finora
- An Approach To Anemic PatientDocumento79 pagineAn Approach To Anemic PatientHussain AzharNessuna valutazione finora
- Acute Renal FailureDocumento120 pagineAcute Renal FailureHussain AzharNessuna valutazione finora
- ABG S Final and Last TouchDocumento88 pagineABG S Final and Last TouchHussain AzharNessuna valutazione finora
- Acute Exacerbation of COPDDocumento14 pagineAcute Exacerbation of COPDMohammad AliNessuna valutazione finora
- Acrf CDocumento70 pagineAcrf CHussain AzharNessuna valutazione finora
- Protocol Book BWCT DominiqueS 2Documento126 pagineProtocol Book BWCT DominiqueS 2N AaNessuna valutazione finora
- Venous Thromboembolic DiseaseDocumento262 pagineVenous Thromboembolic DiseasesamNessuna valutazione finora
- Cor Pulmonale: Peter Celec P Ete Rcelec at GM Ail. Com W W W. Imbm. SKDocumento108 pagineCor Pulmonale: Peter Celec P Ete Rcelec at GM Ail. Com W W W. Imbm. SKAppry M SilabanNessuna valutazione finora
- ICU One Pager - Pulmonary Embolism RX PDFDocumento1 paginaICU One Pager - Pulmonary Embolism RX PDFAbdul RaufNessuna valutazione finora
- Tep Nejm 2022Documento13 pagineTep Nejm 2022Jorge CastilloNessuna valutazione finora
- Alcohol Withdrawal - Epidemiology, Clinical Manifestations, Course, Assessment, and Diagnosis - UpToDateDocumento22 pagineAlcohol Withdrawal - Epidemiology, Clinical Manifestations, Course, Assessment, and Diagnosis - UpToDateSanti Herrera100% (1)
- EmbolismDocumento2 pagineEmbolismShannen Joyce FloresNessuna valutazione finora
- Right Ovarian Vein Thrombosis (Ovt) - A Rare Presentation of Abdominal PainDocumento4 pagineRight Ovarian Vein Thrombosis (Ovt) - A Rare Presentation of Abdominal PainIJAR JOURNALNessuna valutazione finora
- Pi Anterior ResectionDocumento16 paginePi Anterior ResectionEnika Natalia Christi TilaarNessuna valutazione finora
- Radiology CWRU Medical Student Elective Week 1Documento112 pagineRadiology CWRU Medical Student Elective Week 1Yopi SimargiNessuna valutazione finora
- Pulmonary Hypertension: Introduction To Cor PulmonaleDocumento16 paginePulmonary Hypertension: Introduction To Cor PulmonaleJisha JanardhanNessuna valutazione finora
- Deep Vein Thrombosis FlyerDocumento2 pagineDeep Vein Thrombosis FlyerMuhammad Reza Syahli PiliangNessuna valutazione finora
- Diagnosis of Pulmonary Embolism During PregnancyDocumento9 pagineDiagnosis of Pulmonary Embolism During PregnancyFátima AlmeidaNessuna valutazione finora
- Respiratory System BOFDocumento27 pagineRespiratory System BOFBenjamin NelsonNessuna valutazione finora
- Patient Safety Curriculum: Improving A Critical Dimension of Quality in Health CareDocumento19 paginePatient Safety Curriculum: Improving A Critical Dimension of Quality in Health CareClaire Angelie RuayaNessuna valutazione finora
- Cardio PDFDocumento94 pagineCardio PDFSalwaNessuna valutazione finora
- Causes and Investigation of Shock: Learning ObjectivesDocumento3 pagineCauses and Investigation of Shock: Learning Objectivesstef lopezNessuna valutazione finora
- An Update Management of Acute Ischemic Stroke: SurotoDocumento36 pagineAn Update Management of Acute Ischemic Stroke: SurotoShinta DianNessuna valutazione finora
- Perioperatif Nursing PDFDocumento93 paginePerioperatif Nursing PDFNurvanny HusnaNessuna valutazione finora
- Lung Scan: Safuan Awang Nuclear MedicineDocumento19 pagineLung Scan: Safuan Awang Nuclear MedicineVeraaaNessuna valutazione finora