Potrebbero piacerti anche
- Ventricular Septal DefectDocumento8 pagineVentricular Septal DefectMarina RotaruNessuna valutazione finora
- Malnutrition in Children For PDR III - PediaDocumento24 pagineMalnutrition in Children For PDR III - PediaJaniel King100% (1)
- Situational Analysis of Public Health Nursing Personnel in IndiaDocumento60 pagineSituational Analysis of Public Health Nursing Personnel in IndiaTamilNurse.com100% (1)
- Idiophatic Thrombocytopenic Purpura (ITP) in PregnancyDocumento27 pagineIdiophatic Thrombocytopenic Purpura (ITP) in PregnancyAdietya Bima PrakasaNessuna valutazione finora
- Pregnancy Uterus Fetus Embryo: Morbidity Selectively Reduce Multiple PregnancyDocumento4 paginePregnancy Uterus Fetus Embryo: Morbidity Selectively Reduce Multiple Pregnancynyzgirl17Nessuna valutazione finora
- Case StudyDocumento48 pagineCase Studysimbarashe tangwadzanaNessuna valutazione finora
- India's Growing Cervical Cancer EpidemicDocumento54 pagineIndia's Growing Cervical Cancer EpidemicJetty Elizabeth JoseNessuna valutazione finora
- Live Preterm Baby Delivered NSDDocumento13 pagineLive Preterm Baby Delivered NSDKristine Anne SorianoNessuna valutazione finora
- Intrauterine Growth Restriction IUGR: TH THDocumento2 pagineIntrauterine Growth Restriction IUGR: TH THZahra AlaradiNessuna valutazione finora
- Neonatal Jaundice Guide: Causes, Symptoms, DiagnosisDocumento3 pagineNeonatal Jaundice Guide: Causes, Symptoms, DiagnosismeidyNessuna valutazione finora
- Report - For MaamDocumento7 pagineReport - For MaamSherchen Antonio-CortesNessuna valutazione finora
- COPD Secondaryto PTBDocumento142 pagineCOPD Secondaryto PTBallexiscampaner100% (2)
- Postpartum Nursing PowerpointDocumento3 paginePostpartum Nursing PowerpointAntonella VitaleNessuna valutazione finora
- Pregnancy Induced HypertensionDocumento52 paginePregnancy Induced HypertensionJoy GloryNessuna valutazione finora
- Ovarian Cysts and Cancer in PregnancyDocumento15 pagineOvarian Cysts and Cancer in Pregnancykarina100% (1)
- Lecture Notes On AphDocumento41 pagineLecture Notes On AphEyob MizanNessuna valutazione finora
- Gestational HypertensionDocumento5 pagineGestational HypertensionJason Jimmy Lee PillayNessuna valutazione finora
- Hirschsprung's DiseaseDocumento3 pagineHirschsprung's DiseaserjalavazoNessuna valutazione finora
- Family As A Unit of CareDocumento5 pagineFamily As A Unit of CareMonsour SalazarNessuna valutazione finora
- Complications of Third Stage of Labour NishaDocumento21 pagineComplications of Third Stage of Labour NishaSonia SapehiaNessuna valutazione finora
- Case Report Tetralogy of Fallot-CompleteDocumento72 pagineCase Report Tetralogy of Fallot-CompleteMaydis stigmaNessuna valutazione finora
- Abnormal Amniotic Fluid LevelsDocumento29 pagineAbnormal Amniotic Fluid LevelsSTAR Plus SerialsNessuna valutazione finora
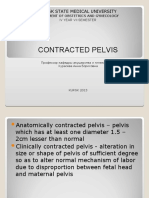
- Contracted Pelvis: Kursk State Medical UniversityDocumento24 pagineContracted Pelvis: Kursk State Medical UniversityLucas Victor AlmeidaNessuna valutazione finora
- Intrauterine Growth RestrictionDocumento5 pagineIntrauterine Growth RestrictionColleen MercadoNessuna valutazione finora
- The Effectiveness of Educational Program On Nurses' Competencies Regarding Pre-Eclampsia Care in Three Hospitals in Sudan2021Documento6 pagineThe Effectiveness of Educational Program On Nurses' Competencies Regarding Pre-Eclampsia Care in Three Hospitals in Sudan2021International Journal of Innovative Science and Research Technology100% (1)
- Case Presentation Hyperemesis Gravidarum Maricar Abonado Midwifery IIDocumento27 pagineCase Presentation Hyperemesis Gravidarum Maricar Abonado Midwifery IIMaricar Crescini AbonadoNessuna valutazione finora
- Neonatal InfectionDocumento56 pagineNeonatal InfectionGanesha Gamma 2017Nessuna valutazione finora
- Causes: Neonatal Jaundice or Neonatal Hyperbilirubinemia, or Neonatal Icterus (From The GreekDocumento7 pagineCauses: Neonatal Jaundice or Neonatal Hyperbilirubinemia, or Neonatal Icterus (From The GreekIzzah100% (1)
- PROM SANJIDA FInal 2Documento32 paginePROM SANJIDA FInal 2Saiful islam RonyNessuna valutazione finora
- Obg Icd-10 Pregnancy, Childbirth, PuerperiumDocumento11 pagineObg Icd-10 Pregnancy, Childbirth, PuerperiumarifianjuariNessuna valutazione finora
- Pre-Eclampsia, Eclampsia and HELLP SyndromeDocumento15 paginePre-Eclampsia, Eclampsia and HELLP SyndromehendraNessuna valutazione finora
- Multifetal Pregnancy: Amr Nadim, MDDocumento36 pagineMultifetal Pregnancy: Amr Nadim, MDsharenNessuna valutazione finora
- Pre and Post PregnancyDocumento23 paginePre and Post PregnancyJitendra ChaudharyNessuna valutazione finora
- WHO Labour Care GuideDocumento34 pagineWHO Labour Care GuideAnkita Singh100% (1)
- Anorectal Malformations: Presented by Khushveer KaurDocumento91 pagineAnorectal Malformations: Presented by Khushveer KaurKataria DavinNessuna valutazione finora
- Risk of Postpartum Infections (39Documento29 pagineRisk of Postpartum Infections (39gerryneutron100% (1)
- High Risk PregnancyDocumento14 pagineHigh Risk PregnancyJezrael PueblosNessuna valutazione finora
- Placenta Previa: AdvertisementDocumento27 paginePlacenta Previa: Advertisementyoung_mizthizah25Nessuna valutazione finora
- PreeclampsiaDocumento14 paginePreeclampsiaHenny NovitasariNessuna valutazione finora
- Opthalmia UmDocumento23 pagineOpthalmia Umnanu-jenuNessuna valutazione finora
- GDM PresetationDocumento26 pagineGDM PresetationYondri Mandaku TasidjawaNessuna valutazione finora
- Managing Nause and Vomiting-Crit-Care-Nurse-2003-Garrett-31-50 PDFDocumento22 pagineManaging Nause and Vomiting-Crit-Care-Nurse-2003-Garrett-31-50 PDFpmuftiaNessuna valutazione finora
- Advantages of Breast FeedingDocumento4 pagineAdvantages of Breast FeedingRollan MaulasNessuna valutazione finora
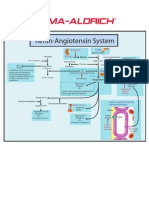
- Renin-Angiotensin SystemDocumento1 paginaRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Abortion and Ectopic PregnancyDocumento3 pagineAbortion and Ectopic PregnancyJefelson Eu Palaña NahidNessuna valutazione finora
- BSc Nursing Exam Questions on Community Health NursingDocumento1 paginaBSc Nursing Exam Questions on Community Health NursingLuwang ChanuNessuna valutazione finora
- Aklan State University Nursing Readings on Pyloric StenosisDocumento5 pagineAklan State University Nursing Readings on Pyloric Stenosisensoooooooooo100% (1)
- Analytical Study of Intrauterine Fetal Death Cases and Associated Maternal ConditionsDocumento5 pagineAnalytical Study of Intrauterine Fetal Death Cases and Associated Maternal ConditionsNurvita WidyastutiNessuna valutazione finora
- Polyhydraminos and OligohydraminosDocumento11 paginePolyhydraminos and OligohydraminosMelissa Catherine ChinNessuna valutazione finora
- IUGRDocumento22 pagineIUGRSairindri SahooNessuna valutazione finora
- Case Presentation: RH Negative PregnancyDocumento19 pagineCase Presentation: RH Negative PregnancyNazee NazreenNessuna valutazione finora
- Threatened AbortionDocumento1 paginaThreatened AbortionKEn PilapilNessuna valutazione finora
- Physiology of the Menstrual CycleDocumento6 paginePhysiology of the Menstrual CyclegmindalanoNessuna valutazione finora
- Operative Delivery: Presenters: Yonas Gudeta (RMHS/402/09)Documento71 pagineOperative Delivery: Presenters: Yonas Gudeta (RMHS/402/09)Jhon Negesse100% (1)
- Rubella and PregnancyDocumento6 pagineRubella and PregnancyKABERA RENENessuna valutazione finora
- Celiac Disease in ChildrenDocumento59 pagineCeliac Disease in Childrend-fbuser-57045067Nessuna valutazione finora
- Developing Theoretical and Conceptual Frameworks and Operational Definition of TermsDocumento44 pagineDeveloping Theoretical and Conceptual Frameworks and Operational Definition of TermsHTCCS BatoCamSurNessuna valutazione finora
- Mastitis Prevention and TreatmentDocumento25 pagineMastitis Prevention and TreatmentGeetha SoundaryaNessuna valutazione finora
- Hypertensive Disorders of Pregnancy: Mohammad Khalandar (116) Megha DDocumento22 pagineHypertensive Disorders of Pregnancy: Mohammad Khalandar (116) Megha DMegha D100% (1)
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Vulvovaginal Atrophy in The CRETA Study The Healthcare Professionals PerceptionDocumento7 pagineVulvovaginal Atrophy in The CRETA Study The Healthcare Professionals PerceptionHugo GutiérrezNessuna valutazione finora
- Dynamic Learning Plan 2-Lesson 2Documento27 pagineDynamic Learning Plan 2-Lesson 2Cyrah OntiverosNessuna valutazione finora
- Analytical Exposition Text Corona Should Be Against Surround UsDocumento2 pagineAnalytical Exposition Text Corona Should Be Against Surround UsRifkyNessuna valutazione finora
- Guideline Mood Australia New Zeland PDFDocumento120 pagineGuideline Mood Australia New Zeland PDFFábio C NetoNessuna valutazione finora
- Warehouse Center Checklist 2Documento5 pagineWarehouse Center Checklist 2Sankar ChinnathambiNessuna valutazione finora
- Gene TherapyDocumento15 pagineGene TherapyRose Mary GeorgeNessuna valutazione finora
- Principles of Health AdminDocumento42 paginePrinciples of Health AdminAnne BattulayanNessuna valutazione finora
- Donald A. Neumann-Kinesiology of The Musculoskeletal SystemDocumento607 pagineDonald A. Neumann-Kinesiology of The Musculoskeletal SystemLuciano Klapisch81% (16)
- Ingles: Estudiante Harold Andrés Bonett SánchezDocumento8 pagineIngles: Estudiante Harold Andrés Bonett SánchezAndrès BonettNessuna valutazione finora
- 004 General Consent English (Front)Documento2 pagine004 General Consent English (Front)عبدالله الرعويNessuna valutazione finora
- Juvenile Rheumatoid Arthritis: Dorothy W. Wortmann, MDDocumento38 pagineJuvenile Rheumatoid Arthritis: Dorothy W. Wortmann, MDLavi GoyalNessuna valutazione finora
- Mole Airlines, Emp. Form. ExcerciseDocumento2 pagineMole Airlines, Emp. Form. ExcerciseKamariah IsmailNessuna valutazione finora
- CHN Assignment (Community Health Nursing)Documento21 pagineCHN Assignment (Community Health Nursing)binjuNessuna valutazione finora
- Training Session Evaluation Form InstructionsDocumento8 pagineTraining Session Evaluation Form Instructionsaaronjules100% (1)
- 31.ergonomic Approach of Modification of Seat - EncDocumento11 pagine31.ergonomic Approach of Modification of Seat - EncSHASHANK ROHITNessuna valutazione finora
- K CC1 102 Hse MSDS 005 - R0 EaDocumento8 pagineK CC1 102 Hse MSDS 005 - R0 EaWalter Gerardo BelluzNessuna valutazione finora
- Week 1 Day 1Documento2 pagineWeek 1 Day 1arens100% (1)
- PDFDocumento7 paginePDFBuloy ReggieNessuna valutazione finora
- Cholera FinalDocumento57 pagineCholera FinalBinayaNessuna valutazione finora
- Sma - Ma Bahasa Inggris Ipa - Ips - Bahasa SecuredDocumento39 pagineSma - Ma Bahasa Inggris Ipa - Ips - Bahasa SecuredJohnson LiuNessuna valutazione finora
- Functional Test and Weight Verification of BalancesDocumento5 pagineFunctional Test and Weight Verification of BalancesMartellRNessuna valutazione finora
- Grade 4 WINS OrientationDocumento2 pagineGrade 4 WINS OrientationChristine FranciscoNessuna valutazione finora
- THHV- 18 G10 ĐỀ NÂNG CAO TỔNG HỢP SỐ 2Documento12 pagineTHHV- 18 G10 ĐỀ NÂNG CAO TỔNG HỢP SỐ 2hCby 28Nessuna valutazione finora
- Mds Periodontics Thesis TopicsDocumento7 pagineMds Periodontics Thesis Topicsamyholmesmanchester100% (2)
- Ethical Decision Making in ResearchDocumento2 pagineEthical Decision Making in ResearchChandraKurniawanNessuna valutazione finora
- Workshop Statistical Methods in Biomedical Research - Nioh - NimsDocumento3 pagineWorkshop Statistical Methods in Biomedical Research - Nioh - NimsSudheerChauhanNessuna valutazione finora
- Nike Vietnam Factory Empowerment Through Information CampaignsDocumento8 pagineNike Vietnam Factory Empowerment Through Information Campaignsvaibhav262Nessuna valutazione finora
- Surya Namaskar BenefitsDocumento16 pagineSurya Namaskar BenefitsMillion Dollar KnowledgeNessuna valutazione finora
- Buku Koding 1Documento74 pagineBuku Koding 1indra_igrNessuna valutazione finora
- Introduction of PhobiaDocumento2 pagineIntroduction of PhobiawoodenskyNessuna valutazione finora