Potrebbero piacerti anche
- EndocrineDocumento144 pagineEndocrineaartiNessuna valutazione finora
- Oestrogen, Progesterone, AndrogensDocumento58 pagineOestrogen, Progesterone, AndrogensTandin SonamNessuna valutazione finora
- Pharmacology of hormonal contraceptionDocumento51 paginePharmacology of hormonal contraceptiondhiyas100% (1)
- All MCN MidtermDocumento207 pagineAll MCN MidtermInah SaritaNessuna valutazione finora
- InfertilityDocumento55 pagineInfertilityFedlu SirajNessuna valutazione finora
- Female Sex Hormones: Natural Estrogens And ProgestinsDocumento30 pagineFemale Sex Hormones: Natural Estrogens And ProgestinsMagdy El-GammalNessuna valutazione finora
- PCOSDocumento38 paginePCOSJitendra ChaudharyNessuna valutazione finora
- Third Quarter Test in Grade 10 ScienceDocumento8 pagineThird Quarter Test in Grade 10 ScienceFroilan AlexNessuna valutazione finora
- Fertility: Assessment and Treatment For People With Fertility ProblemsDocumento4 pagineFertility: Assessment and Treatment For People With Fertility ProblemsPatrick CoghlanNessuna valutazione finora
- Science: Quarter 3 - Module 2Documento16 pagineScience: Quarter 3 - Module 2Fernadez Rodison100% (3)
- Physiotherapy in PCOSDocumento54 paginePhysiotherapy in PCOSAkshaya Nayak100% (3)
- Disorders of The Anterior Pituitary - ESWDocumento78 pagineDisorders of The Anterior Pituitary - ESWpakdejackNessuna valutazione finora
- Introduction to Clinical Reproductive EndocrinologyDa EverandIntroduction to Clinical Reproductive EndocrinologyValutazione: 1 su 5 stelle1/5 (1)
- Thyroid and InfertilityDocumento36 pagineThyroid and InfertilitySairindri SahooNessuna valutazione finora
- 24 Lecture PPT - Reproductive SystemDocumento47 pagine24 Lecture PPT - Reproductive Systemjohnjay3110100% (2)
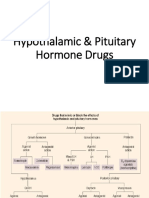
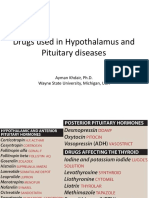
- Hypothalamic & Pituitary Hormone DrugsDocumento29 pagineHypothalamic & Pituitary Hormone DrugsDylan MansillaNessuna valutazione finora
- Placenta Previa Case StudyDocumento59 paginePlacenta Previa Case Studyjuel_navarro88% (33)
- Pediatric Endocrinology Review MCQsDocumento104 paginePediatric Endocrinology Review MCQsTirou100% (1)
- Practice Test MCNDocumento36 paginePractice Test MCNIriel NadongaNessuna valutazione finora
- MCQs For MRCOG Part 1 A Self-Assessment Guide PDF BookDocumento118 pagineMCQs For MRCOG Part 1 A Self-Assessment Guide PDF BookAhmed Abdelmonsef Albashatly86% (14)
- Menstrual CycleDocumento41 pagineMenstrual CyclesharimileeratnamNessuna valutazione finora
- OVARIAN STIMULANTS AND OXYTOCICS - PPTX - 22.04.2021 - Dr. SSDocumento43 pagineOVARIAN STIMULANTS AND OXYTOCICS - PPTX - 22.04.2021 - Dr. SSRashitha NalarangaNessuna valutazione finora
- Endocrinology of PregnancyDocumento68 pagineEndocrinology of PregnancySht SristiNessuna valutazione finora
- 2019 Gonadal Hormones-3Documento197 pagine2019 Gonadal Hormones-3Vishwajeet RaneNessuna valutazione finora
- A. Introduction: 1. BackgroundDocumento4 pagineA. Introduction: 1. BackgroundAndi NurhidayahNessuna valutazione finora
- GNRH and GonadotropinsDocumento47 pagineGNRH and Gonadotropinskaleab AlemayehuNessuna valutazione finora
- Infertility NirwenDocumento55 pagineInfertility Nirwenpok yeahNessuna valutazione finora
- EndocrinologyDocumento21 pagineEndocrinologySANCHAYEETANessuna valutazione finora
- Kuliah PK2 TESKehamilanJULI2010Documento38 pagineKuliah PK2 TESKehamilanJULI2010Fetty NataliaNessuna valutazione finora
- Hypothalamic and Pituitary Drugs (Autosaved)Documento41 pagineHypothalamic and Pituitary Drugs (Autosaved)mug ashNessuna valutazione finora
- Assisted Reproductive TechnologyDocumento41 pagineAssisted Reproductive Technologyshanty Olivia jasirwanNessuna valutazione finora
- Ovarian CycleDocumento78 pagineOvarian CyclefasicaregroupNessuna valutazione finora
- Estrus SynchronizationDocumento27 pagineEstrus SynchronizationMuhammad NaeemNessuna valutazione finora
- Drugs Affecting The FemaleDocumento32 pagineDrugs Affecting The FemaleLule Allan PhillipNessuna valutazione finora
- InfertilityDocumento18 pagineInfertilityphuyalaryan666Nessuna valutazione finora
- Reproductive EndocrinologyDocumento95 pagineReproductive EndocrinologySamuel BaidooNessuna valutazione finora
- Anterior Pituitary HormonesDocumento46 pagineAnterior Pituitary Hormonespramod bhaleraoNessuna valutazione finora
- Pharmacology of Sex Hormones: Molly Downing, PHD Clinical Instructor College of Pharmacy Downing.211@Osu - EduDocumento25 paginePharmacology of Sex Hormones: Molly Downing, PHD Clinical Instructor College of Pharmacy Downing.211@Osu - EduKaish DahiyaNessuna valutazione finora
- Pharmacological Control of Reproduction in The Dog and BitchDocumento22 paginePharmacological Control of Reproduction in The Dog and BitchVeterinary TirupathiNessuna valutazione finora
- EndocrinologyDocumento7 pagineEndocrinologyVijith.V.kumarNessuna valutazione finora
- Steroids JenniferKettelDocumento25 pagineSteroids JenniferKettelvinay0717Nessuna valutazione finora
- Infertility Evaluation & CausesDocumento30 pagineInfertility Evaluation & CausesLal KhanNessuna valutazione finora
- Hpo Axis 2019Documento47 pagineHpo Axis 2019Kalai VendanNessuna valutazione finora
- Infertility: Villanueva, Ian Joseph Virata, Marc Jenaro Yabuki, Ukari Yambot, Kathleen KayDocumento13 pagineInfertility: Villanueva, Ian Joseph Virata, Marc Jenaro Yabuki, Ukari Yambot, Kathleen KayBea SamonteNessuna valutazione finora
- The Hypothalamic-Pituitary-Endocrine AxisDocumento46 pagineThe Hypothalamic-Pituitary-Endocrine Axiskaleab AlemayehuNessuna valutazione finora
- The Biochemical Changes During PregnancyDocumento21 pagineThe Biochemical Changes During PregnancyHUAWEI HUAWEINessuna valutazione finora
- #4 Hypothalamic & Pituitary Hormones 7 PDFDocumento7 pagine#4 Hypothalamic & Pituitary Hormones 7 PDFOmar BasimNessuna valutazione finora
- Med. Therapy4Documento237 pagineMed. Therapy4mjbw54bk2xNessuna valutazione finora
- Notes Infertility Delayed PubertyDocumento9 pagineNotes Infertility Delayed PubertyTONY GO AWAYNessuna valutazione finora
- Female Reproductive System DrugsDocumento84 pagineFemale Reproductive System DrugsPrincess C. SultanNessuna valutazione finora
- The Menstrual Cycle: Dr. Milvan Hadi, M. Ked (Og), SpogDocumento41 pagineThe Menstrual Cycle: Dr. Milvan Hadi, M. Ked (Og), SpogEvi Liana BahriahNessuna valutazione finora
- Reproductive Endocrinology, by Prof - Dr.Vesna Antovska PHD 2023Documento50 pagineReproductive Endocrinology, by Prof - Dr.Vesna Antovska PHD 2023Vesna AntovskaNessuna valutazione finora
- 1 Pituitary and Thyroid PharmacologyDocumento64 pagine1 Pituitary and Thyroid PharmacologyZaina MasriNessuna valutazione finora
- Ovulation Bandung-Prof AnwarDocumento24 pagineOvulation Bandung-Prof AnwarFerio Joelian ChandraNessuna valutazione finora
- Follicle Stimulating HormoneDocumento13 pagineFollicle Stimulating HormoneAgustinus SuryaNessuna valutazione finora
- She PlusDocumento2 pagineShe PlusHarjinder SinghNessuna valutazione finora
- The Hypothalamus and Pituitary GlandDocumento71 pagineThe Hypothalamus and Pituitary GlandRujha Haniena Ahmad RidzuanNessuna valutazione finora
- The Pituitary Gland Phamela Joy S. Alvarez Anatomic and Physiologic OverviewDocumento27 pagineThe Pituitary Gland Phamela Joy S. Alvarez Anatomic and Physiologic OverviewEdelrose LapitanNessuna valutazione finora
- Puberty and The HPG AxisDocumento36 paginePuberty and The HPG AxiskjhkaNessuna valutazione finora
- Biochemical Investigation of Infertile Couple-My PresentationDocumento91 pagineBiochemical Investigation of Infertile Couple-My PresentationOlukoyejo OluwaboriNessuna valutazione finora
- INFERTILITYDocumento30 pagineINFERTILITYShagun TyagiNessuna valutazione finora
- Management of Infertile CoupleDocumento29 pagineManagement of Infertile CoupleSaneem AnwerNessuna valutazione finora
- Female Reproductive Hormones and the Menstrual CycleDocumento32 pagineFemale Reproductive Hormones and the Menstrual Cycleruth thauladanNessuna valutazione finora
- Uspi HCGDocumento1 paginaUspi HCGrcballaNessuna valutazione finora
- Pemicu 3: Siklus Hidup 2014Documento54 paginePemicu 3: Siklus Hidup 2014exxxxooooNessuna valutazione finora
- Hyopthalamus and PituitaryDocumento45 pagineHyopthalamus and PituitaryJalil HaddadinNessuna valutazione finora
- Oral OvulogensDocumento36 pagineOral OvulogensSrilakshmiNessuna valutazione finora
- Biochemical Changes During PregnancyDocumento15 pagineBiochemical Changes During Pregnancyz100% (1)
- Fertility Preservation LectureDocumento33 pagineFertility Preservation LectureDr. Abha MajumdarNessuna valutazione finora
- Case Analaysis On infertility-BALLON-Karlo CDocumento4 pagineCase Analaysis On infertility-BALLON-Karlo CMelinda Cariño BallonNessuna valutazione finora
- Hormones in Reproduction: Presented To: Dr. Akhtar Rasool Presented By: M Tayyab 2012-VA-300Documento17 pagineHormones in Reproduction: Presented To: Dr. Akhtar Rasool Presented By: M Tayyab 2012-VA-300javeria choudharyNessuna valutazione finora
- Chemical Coordination and Integration Chemical Coordination and IntegrationDocumento7 pagineChemical Coordination and Integration Chemical Coordination and IntegrationAkash AbbarapuNessuna valutazione finora
- Female Reproductive System and Childbirth ProcessesDocumento64 pagineFemale Reproductive System and Childbirth ProcessesIvory SantiagoNessuna valutazione finora
- Biology 30 Exemplars 2008Documento85 pagineBiology 30 Exemplars 2008aaron93Nessuna valutazione finora
- Armando Menstrual CycleDocumento2 pagineArmando Menstrual CycleMatthew PinedaNessuna valutazione finora
- First QuizDocumento3 pagineFirst QuizJosal SinonNessuna valutazione finora
- Does Testosterone Have A Role in Erectile Function?: Review AJM Theme Issue: Men's HealthDocumento10 pagineDoes Testosterone Have A Role in Erectile Function?: Review AJM Theme Issue: Men's HealthNandia SeptiyoriniNessuna valutazione finora
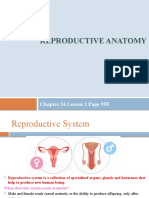
- Reproductive Anatomy: Chapter 34 Lesson 1 Page 958Documento13 pagineReproductive Anatomy: Chapter 34 Lesson 1 Page 958JanaNessuna valutazione finora
- LPL-ROHINI-INFERTILITY-PANELDocumento2 pagineLPL-ROHINI-INFERTILITY-PANELTarunNessuna valutazione finora
- Embryo TransferDocumento21 pagineEmbryo TransferMARCO ANTONIO CABRERA PASCACIONessuna valutazione finora
- Role of Anti-Fertility Medicinal Plants On Male & Female ReproductionDocumento22 pagineRole of Anti-Fertility Medicinal Plants On Male & Female ReproductionMasamune SoraNessuna valutazione finora
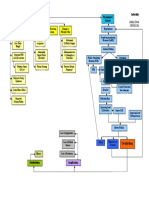
- Infertility Concept MapDocumento1 paginaInfertility Concept Mapnursing concept maps50% (2)
- Bab 15 T4Documento7 pagineBab 15 T4annurkhaliesyaqaisaraNessuna valutazione finora
- Q3W2Documento28 pagineQ3W2pjNessuna valutazione finora
- DAMS CRS - Obstetrics & Gynaecology (DAMS Comprehensive Review Series) - DAMSDocumento36 pagineDAMS CRS - Obstetrics & Gynaecology (DAMS Comprehensive Review Series) - DAMSAbhisek ChatterjeeNessuna valutazione finora
- Flow Chart For Menstrual Cycle: © WWW - Teachitscience.co - Uk 2016 25764 Page 1 of 2Documento2 pagineFlow Chart For Menstrual Cycle: © WWW - Teachitscience.co - Uk 2016 25764 Page 1 of 2SarahNessuna valutazione finora
- Maternal and Child Nursing Care 3rd Edition London Test BankDocumento11 pagineMaternal and Child Nursing Care 3rd Edition London Test BankSerenaNessuna valutazione finora
- Cap.1 - Hypothalamic-Pituitary Sistem 2018 - 2019Documento23 pagineCap.1 - Hypothalamic-Pituitary Sistem 2018 - 2019Razvan GeorgeNessuna valutazione finora
- Semen Practical BiochemDocumento51 pagineSemen Practical BiochemFarahh ArshadNessuna valutazione finora
- Snibe Maglumi Estradiol CliaDocumento4 pagineSnibe Maglumi Estradiol CliaFateh AzwiNessuna valutazione finora