Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Colloidal Silvervs MonkeypoxDocumento20 pagineColloidal Silvervs MonkeypoxJed BatistaNessuna valutazione finora
- Safety Practices And: Sports InjuryDocumento27 pagineSafety Practices And: Sports InjuryRaeven FranciscoNessuna valutazione finora
- ORAL MANIFESTATIONS OF SYSTEMIC DISEASES Part 1Documento97 pagineORAL MANIFESTATIONS OF SYSTEMIC DISEASES Part 1Shreya singhNessuna valutazione finora
- Medical MCQ Center Tuberculosis MCQsDocumento4 pagineMedical MCQ Center Tuberculosis MCQsBanu KubendiranNessuna valutazione finora
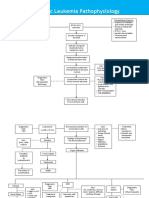
- Acute Lymphoblastic Leukemia Pathophysiology: Predisposing Factors: Etiology: Precipitating FactorsDocumento3 pagineAcute Lymphoblastic Leukemia Pathophysiology: Predisposing Factors: Etiology: Precipitating FactorsKyla ValenciaNessuna valutazione finora
- Diabetes MellitusDocumento29 pagineDiabetes MellitusFourthMolar.com100% (1)
- National Guidelines For IPC in HCF - Final PDFDocumento264 pagineNational Guidelines For IPC in HCF - Final PDFGorav BhallaNessuna valutazione finora
- Group 4 Case Study On Malignant MelanomaDocumento7 pagineGroup 4 Case Study On Malignant MelanomaLance JardiolinNessuna valutazione finora
- 1753-Article Text-39640-3-10-20220815Documento9 pagine1753-Article Text-39640-3-10-20220815Inah SaritaNessuna valutazione finora
- Care of The Patient With COVID-19 COVID Case Study 2Documento3 pagineCare of The Patient With COVID-19 COVID Case Study 2Ashley HernandezNessuna valutazione finora
- Abdominal emergenciesDocumento16 pagineAbdominal emergenciesAdrian BăloiNessuna valutazione finora
- Fever in The Intensive Care Unit - UpToDateDocumento22 pagineFever in The Intensive Care Unit - UpToDateNereida AceitunoNessuna valutazione finora
- Biology Project Reports On HIV ADocumento5 pagineBiology Project Reports On HIV AManish PatidarNessuna valutazione finora
- MD in General Medicine (Revised)Documento28 pagineMD in General Medicine (Revised)Mayank ParasharNessuna valutazione finora
- Questionnaires of ADHD ComorbidityDocumento2 pagineQuestionnaires of ADHD ComorbidityShahar TaorNessuna valutazione finora
- 2 Dupuytrens ContractureDocumento22 pagine2 Dupuytrens ContractureAnonymous m1cmyrNessuna valutazione finora
- St. Paul University Dumaguete College of Nursing ISO 9001Documento6 pagineSt. Paul University Dumaguete College of Nursing ISO 9001Seth Khalil LardausNessuna valutazione finora
- Hepatitis C PHD ThesisDocumento8 pagineHepatitis C PHD Thesisafkogftet100% (2)
- Gerd GuidelineDocumento5 pagineGerd GuidelineBenny TrisaktyariNessuna valutazione finora
- A LZHEIMER'SDocumento9 pagineA LZHEIMER'SPaul Mark PilarNessuna valutazione finora
- Diabetes Mellitus Classification and Diagnostic CriteriaDocumento36 pagineDiabetes Mellitus Classification and Diagnostic Criteriaplogiojayr8340Nessuna valutazione finora
- Manajemen efek samping terapi pasien paliatifDocumento2 pagineManajemen efek samping terapi pasien paliatifFikria Nawaf AuliaNessuna valutazione finora
- Mcguckin 2004Documento4 pagineMcguckin 2004noviaNessuna valutazione finora
- Ritumalta Answers ImciDocumento3 pagineRitumalta Answers ImciJess RitumaltaNessuna valutazione finora
- QUESTIONAIRE Research Final PDFDocumento2 pagineQUESTIONAIRE Research Final PDFAli AfaqNessuna valutazione finora
- Chronic Kidney Disease LIFA FixxxDocumento19 pagineChronic Kidney Disease LIFA FixxxMuzdalifa MohamadNessuna valutazione finora
- DD DemensiaDocumento25 pagineDD DemensiaPutri HarahapNessuna valutazione finora
- 20 Year Old Woman (Case Study) Health AssessmentDocumento2 pagine20 Year Old Woman (Case Study) Health AssessmentJeahannNessuna valutazione finora
- Severe - Acute - Respiratory - Syndrome - Coronavirus - 2 WikiDocumento30 pagineSevere - Acute - Respiratory - Syndrome - Coronavirus - 2 WikiUnggul YudhaNessuna valutazione finora
- Dr. Liliek, Sp. J - Cardiac ArrestDocumento25 pagineDr. Liliek, Sp. J - Cardiac Arrestdhika2496Nessuna valutazione finora