Potrebbero piacerti anche
- Febrile SeizureDocumento6 pagineFebrile SeizurepipimseptianaNessuna valutazione finora
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Depression in The ElderlyDocumento23 pagineDepression in The Elderlylovelots1234Nessuna valutazione finora
- Pleurisy, A Simple Guide To The Condition, Treatment And Related ConditionsDa EverandPleurisy, A Simple Guide To The Condition, Treatment And Related ConditionsNessuna valutazione finora
- Ebola Presentation Ab-5 2Documento21 pagineEbola Presentation Ab-5 2api-302080035Nessuna valutazione finora
- Management of Tuberculosis: A guide for clinicians (eBook edition)Da EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Nessuna valutazione finora
- Acute BronchitisDocumento38 pagineAcute BronchitisNikko MelencionNessuna valutazione finora
- 1 Typhoid FeverDocumento14 pagine1 Typhoid FeverWildan YogaNessuna valutazione finora
- Dengue Fever Signs, Symptoms, and PreventionDocumento9 pagineDengue Fever Signs, Symptoms, and PreventionKyla BalboaNessuna valutazione finora
- Cardiac NSG DiagnosisDocumento5 pagineCardiac NSG DiagnosisShreyas WalvekarNessuna valutazione finora
- PCAP-C Endorsement NotesDocumento2 paginePCAP-C Endorsement NotesLorraine GambitoNessuna valutazione finora
- PneumoniaDocumento19 paginePneumoniagopscharanNessuna valutazione finora
- Acute Dyspnea First RevisionDocumento56 pagineAcute Dyspnea First RevisionAradhanaRamchandaniNessuna valutazione finora
- Community Acquired PneumoniaDocumento28 pagineCommunity Acquired Pneumoniadionisiusvrm100% (1)
- MeaslesDocumento32 pagineMeaslesYum C100% (2)
- Dengue Fever: Causes, Symptoms and PreventionDocumento7 pagineDengue Fever: Causes, Symptoms and PreventionAmber Hope PonsicaNessuna valutazione finora
- CasestudyutiDocumento21 pagineCasestudyutidael_05Nessuna valutazione finora
- Asthma: Chronic Inflammatory Airway DiseaseDocumento22 pagineAsthma: Chronic Inflammatory Airway DiseaseAnna EmNessuna valutazione finora
- Case Study Elective1Documento32 pagineCase Study Elective1Jhem SiribanNessuna valutazione finora
- Case Study (Asthma)Documento3 pagineCase Study (Asthma)AIM100% (1)
- Fluid ElectrolyteDocumento115 pagineFluid ElectrolytePaul EbenezerNessuna valutazione finora
- Acute Glomerulonephritis Case StudyDocumento6 pagineAcute Glomerulonephritis Case StudyjakerzNessuna valutazione finora
- Concept Map Meningitis TheoryDocumento3 pagineConcept Map Meningitis TheoryMia AuliaNessuna valutazione finora
- STEM Activity Plan and Patient CaseDocumento8 pagineSTEM Activity Plan and Patient CaseJay Villasoto100% (1)
- Viral Exanthem (Main)Documento94 pagineViral Exanthem (Main)Starlet Rhonadez Bito-onon OrielNessuna valutazione finora
- E-cigarette Awareness and Use in NYC Young AdultsDocumento59 pagineE-cigarette Awareness and Use in NYC Young AdultsAltaf KhaanNessuna valutazione finora
- Ebola Virus: Deadly Hemorrhagic FeverDocumento16 pagineEbola Virus: Deadly Hemorrhagic FeverSisilia AlfinaNessuna valutazione finora
- Pathophysiology of Tuberculosis: Group 5 Latosa, Selene Lee, Guk Lim, Johanna Magalona, Stephen Mendoza, ColeenDocumento22 paginePathophysiology of Tuberculosis: Group 5 Latosa, Selene Lee, Guk Lim, Johanna Magalona, Stephen Mendoza, ColeenAlexander Santiago ParelNessuna valutazione finora
- Cavite State University: I. ObjectivesDocumento7 pagineCavite State University: I. ObjectivesChamy CruzNessuna valutazione finora
- Recurrent PAF Case StudyDocumento3 pagineRecurrent PAF Case StudyDanae Kristina Natasia BangkanNessuna valutazione finora
- Pertussis Case Definition and Investigation PresentationDocumento62 paginePertussis Case Definition and Investigation PresentationMuhammad Jahari Supianto100% (1)
- Hemorrhagic Cerebro Vascular DiseaseDocumento37 pagineHemorrhagic Cerebro Vascular Diseasejbvaldez100% (1)
- Urinary Tract Infections in ChildrenDocumento56 pagineUrinary Tract Infections in ChildrenmedpedshospitalistNessuna valutazione finora
- Chronic Bronchitis GuideDocumento5 pagineChronic Bronchitis GuideJemalyn M. Saludar100% (2)
- Myasthenia Gravis 2Documento8 pagineMyasthenia Gravis 2IvyBanezNessuna valutazione finora
- Group 5 - Hemodialysis - Chronic Kidney FailureDocumento31 pagineGroup 5 - Hemodialysis - Chronic Kidney FailureKimberly Abella CabreraNessuna valutazione finora
- Dengue Breakbone Fever Case StudyDocumento53 pagineDengue Breakbone Fever Case StudyLeilani Rodriguez AmpoNessuna valutazione finora
- Buerger's DiseaseDocumento4 pagineBuerger's DiseasesweetyjonasNessuna valutazione finora
- Animal Bites Approach GuideDocumento39 pagineAnimal Bites Approach GuideNetii FarhatiNessuna valutazione finora
- Bipolar Brochure English FINAL 150109 PDFDocumento9 pagineBipolar Brochure English FINAL 150109 PDFIka M. HendrajayaNessuna valutazione finora
- Measles (Rubeola) VirusDocumento16 pagineMeasles (Rubeola) Virusstudymedic100% (1)
- City of Manila (Formerly City College of Manila) Mehan Gardens, ManilaDocumento8 pagineCity of Manila (Formerly City College of Manila) Mehan Gardens, Manilaicecreamcone_201Nessuna valutazione finora
- Biliary AtresiaDocumento25 pagineBiliary Atresiajulius billiNessuna valutazione finora
- Bronchiolitis Clinical Practice GuidelineDocumento21 pagineBronchiolitis Clinical Practice GuidelineJuwita PratiwiNessuna valutazione finora
- Community-Acquired Pneumonia GuideDocumento37 pagineCommunity-Acquired Pneumonia GuideKristine-Joy Legaspi FrancoNessuna valutazione finora
- Predisposing Conditions, Management and Prevention of Chronic Kidney DiseaseDocumento52 paginePredisposing Conditions, Management and Prevention of Chronic Kidney DiseaseSaad MotawéaNessuna valutazione finora
- Management of Asthma ExacerbationDocumento13 pagineManagement of Asthma ExacerbationAini Shofa HaniahNessuna valutazione finora
- Otitis Media Clinical PresentationDocumento14 pagineOtitis Media Clinical PresentationIvan PathfinderNessuna valutazione finora
- Au Di Minor Case Study Myasthenia GravisDocumento17 pagineAu Di Minor Case Study Myasthenia Gravisapi-301816885Nessuna valutazione finora
- Acute Glomerulonephritis: Group 8 PresentationDocumento25 pagineAcute Glomerulonephritis: Group 8 PresentationcollinsmagNessuna valutazione finora
- Guillain-Barre Syndrome (GBS)Documento34 pagineGuillain-Barre Syndrome (GBS)api-19916399Nessuna valutazione finora
- Autonomic HyperreflexiaDocumento3 pagineAutonomic HyperreflexiaGibe BebitaNessuna valutazione finora
- MCI Drill Sample ScenariosDocumento8 pagineMCI Drill Sample ScenariosDarylNessuna valutazione finora
- Myxedema ComaDocumento14 pagineMyxedema ComaBing Bing LNessuna valutazione finora
- Intracerebral HemorrageDocumento13 pagineIntracerebral HemorrageChristian JuarezNessuna valutazione finora
- Nursing care of Clients in Emergency Situations - 1Documento48 pagineNursing care of Clients in Emergency Situations - 1Danica FrancoNessuna valutazione finora
- Shock Concept MapDocumento2 pagineShock Concept MapElizabeth GarretsonNessuna valutazione finora
- Schematic Diagram BA HAP HRDocumento2 pagineSchematic Diagram BA HAP HRMika MinsalanNessuna valutazione finora
- Swine FluDocumento34 pagineSwine FluMuhammad Alauddin SarwarNessuna valutazione finora
- BY: Dr. Muhammad Alauddin Sarwar Resident: Mahayal General Hospital KSA and Qatar Hospital Karachi, PakistanDocumento20 pagineBY: Dr. Muhammad Alauddin Sarwar Resident: Mahayal General Hospital KSA and Qatar Hospital Karachi, PakistanMuhammad Alauddin SarwarNessuna valutazione finora
- MeningitisDocumento26 pagineMeningitisMuhammad Alauddin Sarwar100% (5)
- Mitral StenosisDocumento17 pagineMitral StenosisMuhammad Alauddin Sarwar100% (8)
- Acute Coronary SyndromeDocumento24 pagineAcute Coronary SyndromeMuhammad Alauddin Sarwar100% (8)
- Malaria PublisshedDocumento28 pagineMalaria PublisshedMuhammad Alauddin Sarwar100% (9)
- BY: Dr. Muhammad Alauddin Sarwar (MBBS) Sindh Government Qatar Hospital, Karachi, PakistanDocumento33 pagineBY: Dr. Muhammad Alauddin Sarwar (MBBS) Sindh Government Qatar Hospital, Karachi, PakistanMuhammad Alauddin SarwarNessuna valutazione finora
- A Suburban Fairy Tale1919 PDFDocumento4 pagineA Suburban Fairy Tale1919 PDFApuntesIstharNessuna valutazione finora
- Muscle and Tendon Injuries - Evaluation and Management (2017, Springer-Verlag Berlin Heidelberg)Documento440 pagineMuscle and Tendon Injuries - Evaluation and Management (2017, Springer-Verlag Berlin Heidelberg)Joaquin Villagra Jara100% (3)
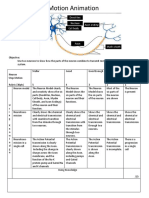
- Neurons Stop Motion AnimationDocumento2 pagineNeurons Stop Motion Animationapi-495006167Nessuna valutazione finora
- The Complex SaraDocumento10 pagineThe Complex SaraFlame10100% (3)
- Comparative Animal Physiology: A Guide to Thermoregulation and MetabolismDocumento7 pagineComparative Animal Physiology: A Guide to Thermoregulation and MetabolismWwwanand111Nessuna valutazione finora
- Rood S ApproachDocumento33 pagineRood S Approachmedway physio teamNessuna valutazione finora
- Pet Agreement and Indemnification RotaDocumento1 paginaPet Agreement and Indemnification RotaLuis Bernal NevaNessuna valutazione finora
- A Kingdom of Blood and Betrayal - Holly ReneeDocumento250 pagineA Kingdom of Blood and Betrayal - Holly ReneeViolet MirzaNessuna valutazione finora
- Balinese Cat Breed Profile: Characteristics, Care, Health and MoreDocumento23 pagineBalinese Cat Breed Profile: Characteristics, Care, Health and MoreprosvetiteljNessuna valutazione finora
- GCC Customs Tariff 2017 for Live Animals & Animal ProductsDocumento435 pagineGCC Customs Tariff 2017 for Live Animals & Animal ProductsColin LoboNessuna valutazione finora
- 5090 s14 QP 11 PDFDocumento16 pagine5090 s14 QP 11 PDFruesNessuna valutazione finora
- June 1, (Thursday) 2017Documento10 pagineJune 1, (Thursday) 2017BS Central, Inc. "The Buzz"Nessuna valutazione finora
- 2013 Skin and Wound Infections - StudentDocumento35 pagine2013 Skin and Wound Infections - Studentmicroperadeniya0% (1)
- Animal Farm / Chapter 8 Reading Organizer Sample AnswersDocumento7 pagineAnimal Farm / Chapter 8 Reading Organizer Sample AnswersJacques SnicketNessuna valutazione finora
- Phrases and SentencesDocumento39 paginePhrases and SentencesGhie Yambao SarmientoNessuna valutazione finora
- Efa 2009 UploadDocumento87 pagineEfa 2009 Uploadrobjones21Nessuna valutazione finora
- Ancient Greek Myths and Their OriginsDocumento28 pagineAncient Greek Myths and Their OriginsJenny WoychukNessuna valutazione finora
- Superstitions Micro TeachingDocumento17 pagineSuperstitions Micro Teachingacerca80100% (1)
- GOMERA BSBA FM-1 Gods of EgyptDocumento3 pagineGOMERA BSBA FM-1 Gods of EgyptGOMERA, ENGELONessuna valutazione finora
- Crocheted Uterus PatternDocumento2 pagineCrocheted Uterus Patternweasley123100% (4)
- Types of ClaimsDocumento14 pagineTypes of ClaimsCatherine Joy ManaloNessuna valutazione finora
- Philippine Literature - Ilocos RegionDocumento6 paginePhilippine Literature - Ilocos RegionRj Bengil0% (1)
- One Thousand Magical Herbs and FungiDocumento16 pagineOne Thousand Magical Herbs and FungiSayanSanyal100% (1)
- 7 Principles of Leave No TraceDocumento2 pagine7 Principles of Leave No TraceDiether100% (1)
- Act 147 Veterinary Surgeons Act 1974Documento39 pagineAct 147 Veterinary Surgeons Act 1974Adam Haida & CoNessuna valutazione finora
- Animal RestraintDocumento72 pagineAnimal RestraintNicka VILLANUEVANessuna valutazione finora
- Creative ParkDocumento14 pagineCreative ParkAli SimsekNessuna valutazione finora
- The Porn Circuit - Covenant Eye - DesconocidoDocumento47 pagineThe Porn Circuit - Covenant Eye - DesconocidoirvmacNessuna valutazione finora
- Ethical Guidelines PsychologyDocumento3 pagineEthical Guidelines PsychologyManal_99xoNessuna valutazione finora
- Paket Buffet Umum 2019Documento3 paginePaket Buffet Umum 2019Ikhasul AmalNessuna valutazione finora