Potrebbero piacerti anche
- Case Study 2Documento2 pagineCase Study 2DUDUNG dudongNessuna valutazione finora
- Online Marketing Overview: Jon SummerfieldDocumento14 pagineOnline Marketing Overview: Jon SummerfieldRmsgNessuna valutazione finora
- The PAIN-FREE PROGRAM - A Proven Method To Relieve Back, Neck, Shoulder, and Joint Pain - 0Documento266 pagineThe PAIN-FREE PROGRAM - A Proven Method To Relieve Back, Neck, Shoulder, and Joint Pain - 0heels100% (3)
- Gastric Function TestsDocumento3 pagineGastric Function TestssreekanthpgNessuna valutazione finora
- Paajoy SuccessionDocumento115 paginePaajoy SuccessionamandaNessuna valutazione finora
- Atherosclerosis, DyslipidemiaDocumento83 pagineAtherosclerosis, DyslipidemiaSilvia MudrencoNessuna valutazione finora
- Antidislipidemic DrugsDocumento25 pagineAntidislipidemic DrugsAlda Gitu RahmaNessuna valutazione finora
- ZCA QuixKioskSMSorsogon CutReport All 13062023to20062023Documento2 pagineZCA QuixKioskSMSorsogon CutReport All 13062023to20062023Patricia LacoNessuna valutazione finora
- ZCA SMDaet CutReport All 14062023to20062023Documento2 pagineZCA SMDaet CutReport All 14062023to20062023Patricia LacoNessuna valutazione finora
- Bad PDFCreatorDocumento3 pagineBad PDFCreatorapi-3766300100% (2)
- Mortality (Global)Documento3 pagineMortality (Global)Daniel Angelo ArangoNessuna valutazione finora
- Bukti 1.29.5Documento8 pagineBukti 1.29.5didiNessuna valutazione finora
- Hutts: A Seed Is Sleepy, and A Butterfly Is PatientDocumento40 pagineHutts: A Seed Is Sleepy, and A Butterfly Is PatientHaseeb ToorNessuna valutazione finora
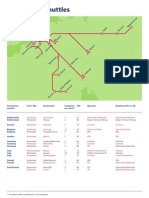
- Kaartrailion Shuttles Maart04Documento1 paginaKaartrailion Shuttles Maart04Meedenken en Doen BVNessuna valutazione finora
- Mymulti Fare MapDocumento1 paginaMymulti Fare MapanandnagsNessuna valutazione finora
- Monitoring ToolsDocumento14 pagineMonitoring ToolsStephanie CastillonNessuna valutazione finora
- Barcelona Estació de França Tarragona Tortosa / Ulldecona Barcelona Estació de França Salou - Port AventuraDocumento2 pagineBarcelona Estació de França Tarragona Tortosa / Ulldecona Barcelona Estació de França Salou - Port AventurafiestajuguetesNessuna valutazione finora
- Figure 10. Junior Highschool Students Question 10 AnswersDocumento1 paginaFigure 10. Junior Highschool Students Question 10 Answerslovely graceNessuna valutazione finora
- GJMH All Rotomoulded Product CatalogueDocumento8 pagineGJMH All Rotomoulded Product CatalogueAbhishek JaiswalNessuna valutazione finora
- Barcelona Estació de França Tarragona Tortosa / Ulldecona Barcelona Estació de França Salou - Port AventuraDocumento2 pagineBarcelona Estació de França Tarragona Tortosa / Ulldecona Barcelona Estació de França Salou - Port AventuraroskienNessuna valutazione finora
- 001bx Sin 261223Documento2 pagine001bx Sin 261223toavuhNessuna valutazione finora
- WMC 2016 Prospectus June 2016 PDFDocumento87 pagineWMC 2016 Prospectus June 2016 PDFAnonymous 0gfzLMYYfXNessuna valutazione finora
- E 03 H 3 JobsDocumento4 pagineE 03 H 3 JobsSarah Azizah WiratamaNessuna valutazione finora
- UndanganDocumento1 paginaUndanganrudianNessuna valutazione finora
- Problem Statements 2023: StoriesDocumento136 pagineProblem Statements 2023: StoriesSuryaprakash MishraNessuna valutazione finora
- 002 002abx Gne 261223Documento4 pagine002 002abx Gne 261223toavuhNessuna valutazione finora
- RCoA - NAP7 - BookDocumento567 pagineRCoA - NAP7 - Bookeric22hkNessuna valutazione finora
- 2022 11 16 RCC Enhanced Brochure FINAL V6Documento21 pagine2022 11 16 RCC Enhanced Brochure FINAL V6Darren ChenNessuna valutazione finora
- Third Quarter Update ReviewDocumento26 pagineThird Quarter Update Reviewelong3102Nessuna valutazione finora
- Grafix DFPM LightdiffuserDocumento4 pagineGrafix DFPM LightdiffuserfiskitNessuna valutazione finora
- Walmart GRRDocumento174 pagineWalmart GRRPatricia DillonNessuna valutazione finora
- Gspaper 1 Book 3Documento57 pagineGspaper 1 Book 3minatoackerman69Nessuna valutazione finora
- Ingredient Vulnerability Assessment BRCDocumento3 pagineIngredient Vulnerability Assessment BRCSherylNessuna valutazione finora
- SGD Evaluation Feedback Q2 2019Documento4 pagineSGD Evaluation Feedback Q2 2019Lugawan ni Bro OfficeNessuna valutazione finora
- Mother Goose Family GuideDocumento4 pagineMother Goose Family GuideKamil KANTARCIOĞLUNessuna valutazione finora
- Ke D Ur Ity Tio Na LH Ea LTH in Su Ran Ce N Ay: Wysynco Trading Company LimitedDocumento2 pagineKe D Ur Ity Tio Na LH Ea LTH in Su Ran Ce N Ay: Wysynco Trading Company LimitedZossia TiexeiraNessuna valutazione finora
- Tema4 PositivePsychologyDocumento16 pagineTema4 PositivePsychologyCristinaNessuna valutazione finora
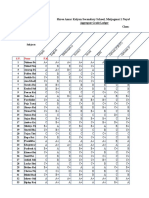
- Shree Amar Kalyan Secondary School, Maijogmai, Ilam: T NV Iro NM en Ed Uc Ati OnDocumento1 paginaShree Amar Kalyan Secondary School, Maijogmai, Ilam: T NV Iro NM en Ed Uc Ati OnDB BhandariNessuna valutazione finora
- 30th Sept Protest - PosterDocumento1 pagina30th Sept Protest - PosteredenmorecdpNessuna valutazione finora
- Dwnload Full Stats Modeling The World 4th Edition Bock Solutions Manual PDFDocumento36 pagineDwnload Full Stats Modeling The World 4th Edition Bock Solutions Manual PDFbuffo.ragman8xns100% (11)
- Using DDL Statements to Create and Manage Tables: license to use this Student GuideฺDocumento40 pagineUsing DDL Statements to Create and Manage Tables: license to use this Student GuideฺSiranjeevi GnanamNessuna valutazione finora
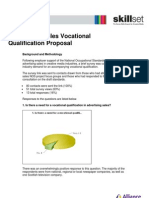
- Ad Sales Qualification ProposalDocumento3 pagineAd Sales Qualification ProposalskillsetsscNessuna valutazione finora
- Achievement ChartDocumento14 pagineAchievement ChartGlenzchie TaguibaoNessuna valutazione finora
- No. Votes For Senator: TA L Senator'S NameDocumento3 pagineNo. Votes For Senator: TA L Senator'S Namekathlyn obayanNessuna valutazione finora
- Co Un T) : Shree Amar Kalyan Secondary School, Maijogmai 1 Nayabazar, IlamDocumento4 pagineCo Un T) : Shree Amar Kalyan Secondary School, Maijogmai 1 Nayabazar, IlamDB BhandariNessuna valutazione finora
- Probability GCSEDocumento49 pagineProbability GCSEDheeraj YadavNessuna valutazione finora
- Aace Company Profile All Verticals 12.04.2024Documento16 pagineAace Company Profile All Verticals 12.04.2024YADVENDRA SINGH TIWARINessuna valutazione finora
- DatasetDocumento341 pagineDatasetSanath Fernando100% (1)
- Ca JHS OneDocumento21 pagineCa JHS OneAmeyaw SamuelNessuna valutazione finora
- PF3 1 Public Spending On Childcare and Early EducationDocumento6 paginePF3 1 Public Spending On Childcare and Early EducationJashandeep MakkarNessuna valutazione finora
- Walt Disney Studios Top Grossing MoviesDocumento7 pagineWalt Disney Studios Top Grossing MoviesBerenice Montiel HernandezNessuna valutazione finora
- Beato - FLS AchievementDocumento9 pagineBeato - FLS AchievementRoedfrey OrtizNessuna valutazione finora
- Salford Suicide Prevention Strategy 2017 22Documento25 pagineSalford Suicide Prevention Strategy 2017 22jose aliNessuna valutazione finora
- Minimally Invasive Caries Treatment: Distributed by StraumannDocumento8 pagineMinimally Invasive Caries Treatment: Distributed by StraumannHassan MohamedNessuna valutazione finora
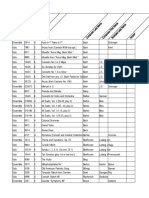
- Solo and Ensemble LibraryDocumento18 pagineSolo and Ensemble LibrarySparibNessuna valutazione finora
- Tabel GrafikDocumento2 pagineTabel Grafikfatmaasri112Nessuna valutazione finora
- UntitledDocumento1 paginaUntitledOtávio CascaesNessuna valutazione finora
- Service: Touareg 2010 Touareg 2015Documento408 pagineService: Touareg 2010 Touareg 2015lognay5Nessuna valutazione finora
- 2017 Generic Lawncare Equipment Quartery Check ListDocumento2 pagine2017 Generic Lawncare Equipment Quartery Check ListCogbillConstructionNessuna valutazione finora
- Ewd 43Documento4 pagineEwd 43Antonio GomezNessuna valutazione finora
- National Standards For Music Education LKDocumento1 paginaNational Standards For Music Education LKMary Maxwell100% (1)
- The Crimson Cowboys: The Remarkable Odyssey of the 1931 Claflin-Emerson ExpeditionDa EverandThe Crimson Cowboys: The Remarkable Odyssey of the 1931 Claflin-Emerson ExpeditionNessuna valutazione finora
- CAP N BiblioDocumento2 pagineCAP N BibliodanradulescuNessuna valutazione finora
- HTAP La VarstniciDocumento16 pagineHTAP La VarstnicidanradulescuNessuna valutazione finora
- CAP N BiblioDocumento2 pagineCAP N BibliodanradulescuNessuna valutazione finora
- Gastrointestinal Fabry DiseaseDocumento14 pagineGastrointestinal Fabry DiseasedanradulescuNessuna valutazione finora
- CV Physical ExaminationDocumento29 pagineCV Physical ExaminationdanradulescuNessuna valutazione finora
- Articol PT Clujul Med.Documento5 pagineArticol PT Clujul Med.danradulescuNessuna valutazione finora
- HTA Guideliness - Esc2007 - SlidesDocumento31 pagineHTA Guideliness - Esc2007 - SlidesdanradulescuNessuna valutazione finora
- Pulmonary Edema: Prepared By: South West Education CommitteeDocumento65 paginePulmonary Edema: Prepared By: South West Education CommitteedanradulescuNessuna valutazione finora
- General: Determination of Heart Rate and Rhythm Determination of The Heart RateDocumento14 pagineGeneral: Determination of Heart Rate and Rhythm Determination of The Heart RatedanradulescuNessuna valutazione finora
- CardiomiopatiiDocumento70 pagineCardiomiopatiidanradulescuNessuna valutazione finora
- VS Noncompact PDFDocumento27 pagineVS Noncompact PDFdanradulescuNessuna valutazione finora
- Critical Analysis REBTDocumento4 pagineCritical Analysis REBTMehar KhanNessuna valutazione finora
- Childhood Sexual Abuse, Relationship Satisfaction, and Sexual Risk Taking in A Community Sample of WomenDocumento9 pagineChildhood Sexual Abuse, Relationship Satisfaction, and Sexual Risk Taking in A Community Sample of WomenScott PymNessuna valutazione finora
- Chulabhorn Graduate Institute Post-Graduate Scholarship Program Scholarship Application Form (For NON-ASEAN Applicants)Documento5 pagineChulabhorn Graduate Institute Post-Graduate Scholarship Program Scholarship Application Form (For NON-ASEAN Applicants)maha AbdulazizNessuna valutazione finora
- Course Reflection Life Drugs and SocietyDocumento3 pagineCourse Reflection Life Drugs and Societyapi-542779175Nessuna valutazione finora
- Book Review: The Five Dysfunctions of A Team by Patrick LencioniDocumento12 pagineBook Review: The Five Dysfunctions of A Team by Patrick LencioniMohammed AbrarNessuna valutazione finora
- Siddha Medicine For BronchitisDocumento2 pagineSiddha Medicine For BronchitisGokul SmartNessuna valutazione finora
- Handwashing Concept NoteDocumento2 pagineHandwashing Concept NoteEmperorr Tau Mtetwa67% (3)
- Anjaneya ShatakamDocumento24 pagineAnjaneya Shatakamsrihita03Nessuna valutazione finora
- Sarivanivatmaulia (2223170001 6a) Worksheet 11Documento3 pagineSarivanivatmaulia (2223170001 6a) Worksheet 11tapdew 25Nessuna valutazione finora
- Las Ro3 Final h9q3w4 8Documento17 pagineLas Ro3 Final h9q3w4 8Randolf CruzNessuna valutazione finora
- Ngampeerapong C 2019Documento12 pagineNgampeerapong C 2019Fauzi SatriaNessuna valutazione finora
- SHS Hope 12 PDFDocumento27 pagineSHS Hope 12 PDFapollo100% (2)
- CHECKLIST Hot and Cold Application WITH RATIONALEDocumento5 pagineCHECKLIST Hot and Cold Application WITH RATIONALEBryle NavoraNessuna valutazione finora
- Bodybuilding ManualDocumento308 pagineBodybuilding ManualM.Emre Doğru100% (2)
- D. Roy - Medicine and Use of MedicineDocumento82 pagineD. Roy - Medicine and Use of Medicinemustakim.martNessuna valutazione finora
- I. Abstract: Nguyen Quynh Anh - GBH200871 - GBH1002Documento8 pagineI. Abstract: Nguyen Quynh Anh - GBH200871 - GBH1002Nguyen Khoi Nguyen (FGW HN)Nessuna valutazione finora
- 0092015020Documento9 pagine0092015020ChloéNessuna valutazione finora
- Collins - Grammar For IELTSDocumento36 pagineCollins - Grammar For IELTSBao HoaNessuna valutazione finora
- Transferring: Bed To StretcherDocumento3 pagineTransferring: Bed To StretcherARUN VNessuna valutazione finora
- Posttraumatic Stress Disorder (PTSD)Documento28 paginePosttraumatic Stress Disorder (PTSD)Karl Angelo MontanoNessuna valutazione finora
- Perilite ExposureDocumento15 paginePerilite ExposureBella Cy Lopez67% (3)
- Compensatory Education: Making-Up For What Your Child Lost: Hertog Education Law, PCDocumento13 pagineCompensatory Education: Making-Up For What Your Child Lost: Hertog Education Law, PCallisonhertogNessuna valutazione finora
- Bravo PSSG Waytan Mary Grace F Assignment 1Documento8 pagineBravo PSSG Waytan Mary Grace F Assignment 1graceNessuna valutazione finora
- Human Cloning and Violation of Human RightDocumento6 pagineHuman Cloning and Violation of Human Rightgaurav singhNessuna valutazione finora
- National Service Training Program Service Learning Program: Help The VulnerableDocumento11 pagineNational Service Training Program Service Learning Program: Help The VulnerableBrunhild BangayanNessuna valutazione finora
- Interview ChecklistDocumento4 pagineInterview ChecklistGreizen John ViloriaNessuna valutazione finora