Potrebbero piacerti anche
- Medical Cert Fitness To Fly PDFDocumento1 paginaMedical Cert Fitness To Fly PDFNafiul IslamNessuna valutazione finora
- Systema For The ElderlyDocumento4 pagineSystema For The ElderlyNicolas Drl100% (1)
- First Quarter Examination Mapeh 8: Raba National High SchoolDocumento2 pagineFirst Quarter Examination Mapeh 8: Raba National High SchoolJay50% (4)
- Ges New Jhs Syllabus Career Technology CCP Curriculum For b7 b10 Draft ZeroDocumento367 pagineGes New Jhs Syllabus Career Technology CCP Curriculum For b7 b10 Draft ZeroElvis Adjei Yamoah100% (1)
- Ana PDFDocumento52 pagineAna PDFCristina Fernández Valencia100% (1)
- (TPSA) : Summary and Explanation PrincipleDocumento7 pagine(TPSA) : Summary and Explanation PrinciplecassNessuna valutazione finora
- ANA Diagnostico IIFTDocumento40 pagineANA Diagnostico IIFTCEAR ReumatologíaNessuna valutazione finora
- Test Instruction Ana EuroimmunDocumento16 pagineTest Instruction Ana EuroimmunSiskawati SuparminNessuna valutazione finora
- DST Final Exam NotesDocumento56 pagineDST Final Exam NoteslmaoheartsNessuna valutazione finora
- Fa 1510 I Uk B PDFDocumento52 pagineFa 1510 I Uk B PDFsurekhaNessuna valutazione finora
- Fa 1510 I Uk B PDFDocumento52 pagineFa 1510 I Uk B PDFsurekhaNessuna valutazione finora
- Cannabis and Mental Health FactsheetDocumento13 pagineCannabis and Mental Health FactsheetEslam El-RefaeNessuna valutazione finora
- Five Year Plans of India..Documento27 pagineFive Year Plans of India..Nalin08100% (11)
- AAK ANA Komplett Kunde PDFDocumento64 pagineAAK ANA Komplett Kunde PDFm parasiteNessuna valutazione finora
- AAK ANA Komplett Kunde PDFDocumento64 pagineAAK ANA Komplett Kunde PDFm parasiteNessuna valutazione finora
- ANA Diagnostics Using Indirect Immunofl UorescenceDocumento52 pagineANA Diagnostics Using Indirect Immunofl UorescenceJael CayetanoNessuna valutazione finora
- Neurology Mosaics Instructions For The Indirect Immunofluorescence TestDocumento24 pagineNeurology Mosaics Instructions For The Indirect Immunofluorescence Testnbiolab6659Nessuna valutazione finora
- PR Pierre Miossec MD PHD Clinical Immunology and Rheumatology Lyon Miossec@Documento23 paginePR Pierre Miossec MD PHD Clinical Immunology and Rheumatology Lyon Miossec@Nam LeeNessuna valutazione finora
- ANA Profiles & Guide To InterpretationDocumento3 pagineANA Profiles & Guide To InterpretationRahul KirkNessuna valutazione finora
- AVNfinal LC2204Documento35 pagineAVNfinal LC2204Davut ÇekmecelioğluNessuna valutazione finora
- Connective Tissue DZDocumento1 paginaConnective Tissue DZAndre GarciaNessuna valutazione finora
- Antinuclear Antibodies (Anas) Antibodies To Extractable Nuclear Antigens (Anti-Enas)Documento8 pagineAntinuclear Antibodies (Anas) Antibodies To Extractable Nuclear Antigens (Anti-Enas)Abdalazeez AlsayedNessuna valutazione finora
- Spesifikasi VIDAS PCDocumento2 pagineSpesifikasi VIDAS PCABD ENOUR BOUALOULNessuna valutazione finora
- Abcam - PEDF ELISA Datasheet - 246535Documento5 pagineAbcam - PEDF ELISA Datasheet - 246535柯砲肚Nessuna valutazione finora
- Antinuclear Antibodies: When To Test and How To Interpret FindingsDocumento4 pagineAntinuclear Antibodies: When To Test and How To Interpret FindingsFariz NurNessuna valutazione finora
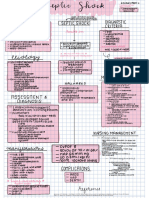
- Septic ShockDocumento2 pagineSeptic ShockmeNessuna valutazione finora
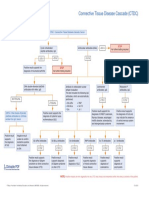
- Connective Tissue Disease CascadeDocumento1 paginaConnective Tissue Disease CascadeYustina BubnovaNessuna valutazione finora
- Coagulopatía Asociada A SepsisDocumento1 paginaCoagulopatía Asociada A SepsisMARIA FERNANDA VALVAS ACERONessuna valutazione finora
- ANA Detection StrategyDocumento1 paginaANA Detection StrategyBassem AhmedNessuna valutazione finora
- MATERI 1 GENETIKA 2019 TugasDocumento65 pagineMATERI 1 GENETIKA 2019 TugasRico RamadhanNessuna valutazione finora
- Alanine Aminotransferase - ADVIA Chemistry - Rev H DXDCM 09008b8380856f9f-1507078406798Documento12 pagineAlanine Aminotransferase - ADVIA Chemistry - Rev H DXDCM 09008b8380856f9f-1507078406798mnemonicsNessuna valutazione finora
- Melamine Test (HPLC GC)Documento5 pagineMelamine Test (HPLC GC)widodoNessuna valutazione finora
- Nse IflashDocumento4 pagineNse IflashNIGHT tubeNessuna valutazione finora
- RNA Therapeutics: How Far Have We Gone?: Maria Francisca Coutinho, Liliana Matos, Juliana Inês Santos, and Sandra AlvesDocumento45 pagineRNA Therapeutics: How Far Have We Gone?: Maria Francisca Coutinho, Liliana Matos, Juliana Inês Santos, and Sandra AlvesIgor BatistaNessuna valutazione finora
- RNA Therapeutics: How Far Have We Gone?: Maria Francisca Coutinho, Liliana Matos, Juliana Inês Santos, and Sandra AlvesDocumento45 pagineRNA Therapeutics: How Far Have We Gone?: Maria Francisca Coutinho, Liliana Matos, Juliana Inês Santos, and Sandra AlvesIgor BatistaNessuna valutazione finora
- Agilent 2100 Kits and ReagentsDocumento2 pagineAgilent 2100 Kits and ReagentsFabian GomezNessuna valutazione finora
- Anticuerpos PDFDocumento1 paginaAnticuerpos PDFOmar Enrique Ocaña GarciaNessuna valutazione finora
- Types of RNA and DNA PuckeringDocumento6 pagineTypes of RNA and DNA PuckeringAman KhanNessuna valutazione finora
- Chemistry: Complete Blood CountDocumento1 paginaChemistry: Complete Blood CountRuet ElahiNessuna valutazione finora
- Meningitis ValuesDocumento1 paginaMeningitis ValuesYukta ThackerNessuna valutazione finora
- 1 Lines EsofagoDocumento33 pagine1 Lines EsofagoClaudia MartínezNessuna valutazione finora
- Amit ReportDocumento3 pagineAmit ReportXlramitNessuna valutazione finora
- Author: Wilsie M. Salas M.DDocumento25 pagineAuthor: Wilsie M. Salas M.DrowenanuquiNessuna valutazione finora
- In Gratitude For mRNA Vaccines: Clinical Implications of Basic ResearchDocumento4 pagineIn Gratitude For mRNA Vaccines: Clinical Implications of Basic ResearchAlizaPinkyNessuna valutazione finora
- Global Profiling of RNA-binding Protein TargetDocumento28 pagineGlobal Profiling of RNA-binding Protein TargetYanjiaoNessuna valutazione finora
- Module 7 - TECHNOLOGY and MTB - RIF Assay (Autosaved)Documento70 pagineModule 7 - TECHNOLOGY and MTB - RIF Assay (Autosaved)Ermias Alemayehu BerisoNessuna valutazione finora
- (Template Only) DSDocumento2 pagine(Template Only) DSMAE ANN MU�OZNessuna valutazione finora
- Catalogue HV Fia 3000Documento6 pagineCatalogue HV Fia 3000Matheus NovaesNessuna valutazione finora
- Abbreviation IndexDocumento1 paginaAbbreviation IndexRocio SandersNessuna valutazione finora
- Lab ProceduresDocumento7 pagineLab Procedureslaurie.charlynjaneNessuna valutazione finora
- Lec 8Documento3 pagineLec 8lilliaNessuna valutazione finora
- 07 MrsSAKSHI 31Y FemaleDocumento4 pagine07 MrsSAKSHI 31Y FemaleRajat SinhaNessuna valutazione finora
- Bio Lec 3Documento2 pagineBio Lec 3lilliaNessuna valutazione finora
- 098 Anti-HCV-IFU-V3.05-en-othersDocumento4 pagine098 Anti-HCV-IFU-V3.05-en-othersPierina DonayreNessuna valutazione finora
- PL95Documento8 paginePL95Untold DarknessNessuna valutazione finora
- Harper S Illustrated Biochemistry by Vic-385-403Documento19 pagineHarper S Illustrated Biochemistry by Vic-385-403DavidNessuna valutazione finora
- Rna RnaDocumento22 pagineRna RnaJNVG XIB BOYSNessuna valutazione finora
- RNL DruDocumento1 paginaRNL DruLanaAmerieNessuna valutazione finora
- Parte 2 BioDocumento150 pagineParte 2 BioPâmella PicançoNessuna valutazione finora
- MCTD 3Documento1 paginaMCTD 3Laksmita Ayu Dewi TetanelNessuna valutazione finora
- 2021 Silicone-Oils ENG MKT273 Rev2 SINGLE-PAGESDocumento4 pagine2021 Silicone-Oils ENG MKT273 Rev2 SINGLE-PAGESTALLAH CHOWHANNessuna valutazione finora
- The RNA Integrity Number (RIN) : IndexDocumento14 pagineThe RNA Integrity Number (RIN) : IndexAli AldosNessuna valutazione finora
- Fertilidad SEMECEDocumento14 pagineFertilidad SEMECEArnoldo FelixNessuna valutazione finora
- Report XLCVDocumento1 paginaReport XLCVmohammad Imtiyaz AnsariNessuna valutazione finora
- The Signifi Cance of Anti-DFS70 in ANA Diagnostics: Does A Positive anti-DFS70 Fi Nding Indicate That No SRA Is Present?Documento2 pagineThe Signifi Cance of Anti-DFS70 in ANA Diagnostics: Does A Positive anti-DFS70 Fi Nding Indicate That No SRA Is Present?sg1192014Nessuna valutazione finora
- Hema Lec311 Week 17 Blood Cell CytochemistryDocumento3 pagineHema Lec311 Week 17 Blood Cell CytochemistryMax RuideraNessuna valutazione finora
- Anti-Dsdna-Ncx Elisa (Igg) Test Instruction: Summary and ExplanationDocumento12 pagineAnti-Dsdna-Ncx Elisa (Igg) Test Instruction: Summary and Explanationanahh ramakNessuna valutazione finora
- Uromodulin ELISA: (Tamm-Horsfall-Glycoprotein)Documento35 pagineUromodulin ELISA: (Tamm-Horsfall-Glycoprotein)m parasiteNessuna valutazione finora
- Uromodulin - ELISA - en 04 - 2016 - VHDocumento17 pagineUromodulin - ELISA - en 04 - 2016 - VHm parasiteNessuna valutazione finora
- Fluorescence Microscopy ResultsDocumento25 pagineFluorescence Microscopy Resultsm parasiteNessuna valutazione finora
- Report (Patient) : ResultDocumento1 paginaReport (Patient) : Resultm parasiteNessuna valutazione finora
- Professional Learning Record Chart YrDocumento11 pagineProfessional Learning Record Chart Yrapi-716050560Nessuna valutazione finora
- Community Health Nursing 2: Philip Jerome A. Flores, RN, MSN LecturerDocumento20 pagineCommunity Health Nursing 2: Philip Jerome A. Flores, RN, MSN LecturerAriane-Gay Cristobal DuranNessuna valutazione finora
- Publicação 2Documento8 paginePublicação 2BrunoNessuna valutazione finora
- 813-Article Text-1261-1-10-20180214Documento5 pagine813-Article Text-1261-1-10-20180214dwiky ramaNessuna valutazione finora
- Effortless Swimming S Workouts: Where To StartDocumento17 pagineEffortless Swimming S Workouts: Where To StartGustavo CastilhoNessuna valutazione finora
- Separation Anxi-WPS OfficeDocumento28 pagineSeparation Anxi-WPS Officedawit alemzewdNessuna valutazione finora
- Week 3 Assignment: Lab: Due Sunday by 11:59pmDocumento7 pagineWeek 3 Assignment: Lab: Due Sunday by 11:59pmEssay NationNessuna valutazione finora
- Effectiveness of The Rehabilitation Program After Colorectal Surgery For Patients With Colorectal Cancer: A Quasi-Experimental StudyDocumento18 pagineEffectiveness of The Rehabilitation Program After Colorectal Surgery For Patients With Colorectal Cancer: A Quasi-Experimental StudyPhattaraladaNessuna valutazione finora
- Chinese GarterDocumento3 pagineChinese Gartereden estrado mendoza100% (1)
- T File To PrintDocumento6 pagineT File To Printanna.mary.arueta.gintoro031202Nessuna valutazione finora
- D2 Presentation Matt Singleton Swiss Re Dementia and InsuranceDocumento13 pagineD2 Presentation Matt Singleton Swiss Re Dementia and InsuranceRishi KumarNessuna valutazione finora
- Unstd-Com 6111 Beef Ground Frozen HalalDocumento2 pagineUnstd-Com 6111 Beef Ground Frozen HalalGagan Sai ReddyNessuna valutazione finora
- One Page Policy Brie1introDocumento2 pagineOne Page Policy Brie1introapi-539369902Nessuna valutazione finora
- The Relationship Between The Duration of Playing Gadget and Mental Emotional State of Elementary School StudentsDocumento4 pagineThe Relationship Between The Duration of Playing Gadget and Mental Emotional State of Elementary School StudentsNurul Fatehah Binti KamaruzaliNessuna valutazione finora
- Neil HillDocumento32 pagineNeil HillAndrés Felipe100% (1)
- All Questions Med SurgDocumento8 pagineAll Questions Med SurgShreya ShindeNessuna valutazione finora
- SIC - 01252 Sickness NotificationDocumento3 pagineSIC - 01252 Sickness NotificationJeannylyn BurgosNessuna valutazione finora
- AAP January 2024 Complete Issue NeoReviewsDocumento71 pagineAAP January 2024 Complete Issue NeoReviewshabibfmNessuna valutazione finora
- Determination of Antioxidant Activity, Total Phenolic, Flavonoid and Alkaloids Content of Pandacaqui (Tabernaemontana Leaf and Flower ExtractsDocumento5 pagineDetermination of Antioxidant Activity, Total Phenolic, Flavonoid and Alkaloids Content of Pandacaqui (Tabernaemontana Leaf and Flower ExtractsGenesis GenesisNessuna valutazione finora
- Effects of A Meal Replacement On Body CompositionDocumento10 pagineEffects of A Meal Replacement On Body CompositionGiffariNessuna valutazione finora
- Complaints Register TemplateDocumento2 pagineComplaints Register Templatewecare4u555Nessuna valutazione finora
- The Role of Health and Education and Economic Growth of PakistanDocumento68 pagineThe Role of Health and Education and Economic Growth of PakistankamilbismaNessuna valutazione finora
- The Mediating Role of Emotional Intelligence in The Employees PerformanceDocumento11 pagineThe Mediating Role of Emotional Intelligence in The Employees PerformanceMårkö ÅlexövåNessuna valutazione finora