Potrebbero piacerti anche
- Dermatoscopy and Skin Cancer, updated edition: A handbook for hunters of skin cancer and melanomaDa EverandDermatoscopy and Skin Cancer, updated edition: A handbook for hunters of skin cancer and melanomaNessuna valutazione finora
- Principles of Management of Soft Tissue SarcomaDocumento33 paginePrinciples of Management of Soft Tissue Sarcomabashiruaminu100% (1)
- The Surgical Anatomy of The Nerve Laryngeal RecurrensDocumento2 pagineThe Surgical Anatomy of The Nerve Laryngeal RecurrensvaNessuna valutazione finora
- Thyroid Cancer Diagnosis and ManagementDocumento45 pagineThyroid Cancer Diagnosis and Managementapi-3704562100% (1)
- Excision of Branchial Cleft CystsDocumento10 pagineExcision of Branchial Cleft Cystssjs315Nessuna valutazione finora
- Skin GraftDocumento38 pagineSkin GraftAndika August100% (1)
- Fracture and Dislocation-Rahardyan Magetsari (2016) PDFDocumento105 pagineFracture and Dislocation-Rahardyan Magetsari (2016) PDFRobertOktaChandraNessuna valutazione finora
- EktremitasDocumento40 pagineEktremitasBram wijayaNessuna valutazione finora
- EGDT SepsisDocumento8 pagineEGDT Sepsissiti fatmalaNessuna valutazione finora
- Mid Face Fractures 1Documento12 pagineMid Face Fractures 1Muh IqbalNessuna valutazione finora
- Anatomi Saraf PeriferDocumento57 pagineAnatomi Saraf PeriferErreli K. KhusumawerdanieNessuna valutazione finora
- Kompartemen SindromDocumento9 pagineKompartemen SindromPutri PratiwiNessuna valutazione finora
- Craniotomy FlapsDocumento41 pagineCraniotomy FlapsKaramsi Gopinath NaikNessuna valutazione finora
- Jaw Tumors: DR - Sudipta Bera PDT 1 Year Plastic and Reconstructive Surgery SSKM & IpgmerDocumento28 pagineJaw Tumors: DR - Sudipta Bera PDT 1 Year Plastic and Reconstructive Surgery SSKM & Ipgmerdevinchi09Nessuna valutazione finora
- FlapDocumento4 pagineFlapMd Ahsanuzzaman PinkuNessuna valutazione finora
- Subtotal ThyroidectomyDocumento26 pagineSubtotal ThyroidectomyJimmyNessuna valutazione finora
- Flaps: Rosallia MegawatiDocumento37 pagineFlaps: Rosallia MegawatiMorinda Daru MurtiNessuna valutazione finora
- Flaps: BY:-Dr. P. Koushik GUIDE: - DR (Brig.) B. B. DograDocumento27 pagineFlaps: BY:-Dr. P. Koushik GUIDE: - DR (Brig.) B. B. DograSumit HadgaonkarNessuna valutazione finora
- Jurnal Tyroid PDFDocumento3 pagineJurnal Tyroid PDFVinnaNessuna valutazione finora
- Tenosynovitis: Dr. Diyar A. SalihDocumento32 pagineTenosynovitis: Dr. Diyar A. SalihsultantraNessuna valutazione finora
- Basic and Special Suturing Techniques in Surgery. Honlap 2Documento57 pagineBasic and Special Suturing Techniques in Surgery. Honlap 2Arif Nurhidayat PrawirohardjoNessuna valutazione finora
- Presentation 1Documento25 paginePresentation 1Nihar ShahNessuna valutazione finora
- Cyst Neck Tumor (DR Bob Andinata)Documento33 pagineCyst Neck Tumor (DR Bob Andinata)Intan Eklesiana NapitupuluNessuna valutazione finora
- Section: Thyroid, Hyperthyroidisme, HypothyroidismeDocumento69 pagineSection: Thyroid, Hyperthyroidisme, HypothyroidismeiikNessuna valutazione finora
- To HerniotomiDocumento16 pagineTo HerniotomikawaishoneNessuna valutazione finora
- Oral LymphangiomaDocumento8 pagineOral LymphangiomasevattapillaiNessuna valutazione finora
- Fraktur Distal HumerusDocumento32 pagineFraktur Distal HumerussyaifularisNessuna valutazione finora
- Cervicofacial LymphangiomasDocumento11 pagineCervicofacial LymphangiomasCharmila Sari100% (1)
- KemoterapiDocumento29 pagineKemoterapiMuammar KadafiNessuna valutazione finora
- Tugas Farmasi: Pembimbing: Yudi Purnomo, S.Si, Apt, M.KesDocumento225 pagineTugas Farmasi: Pembimbing: Yudi Purnomo, S.Si, Apt, M.KesAglalita Jamhur Risia TamaNessuna valutazione finora
- A Case of Thyroglossal CystDocumento23 pagineA Case of Thyroglossal CystArya KepakisanNessuna valutazione finora
- Jurnal CA TyroidDocumento4 pagineJurnal CA TyroidErvina ZelfiNessuna valutazione finora
- Superficial Parotidectomy Through Retrograde Facial Nerve DissectionDocumento8 pagineSuperficial Parotidectomy Through Retrograde Facial Nerve DissectionAnonymous LnWIBo1GNessuna valutazione finora
- Nervus Laryngeus RecurrensDocumento5 pagineNervus Laryngeus RecurrensAri Julian SaputraNessuna valutazione finora
- Sialadenitis: K.Abhinaya. Bds 3 YearDocumento14 pagineSialadenitis: K.Abhinaya. Bds 3 YearAsline JesicaNessuna valutazione finora
- HNSCC Epigenetic LandscapeDocumento16 pagineHNSCC Epigenetic LandscapeSpore FluxNessuna valutazione finora
- Chronic Limb IschemiaDocumento29 pagineChronic Limb IschemiaSadia NaveedNessuna valutazione finora
- Thyroid CancerDocumento39 pagineThyroid CancerFaheem SarwarNessuna valutazione finora
- Thyroid Disorders: Tapan A. Patel Cuong Nguyen Mona JamaldinianDocumento41 pagineThyroid Disorders: Tapan A. Patel Cuong Nguyen Mona Jamaldiniansheila_kohNessuna valutazione finora
- Harvesting STSG: I Gusti Ayu Putri PurwanthiDocumento22 pagineHarvesting STSG: I Gusti Ayu Putri PurwanthiPutri PurwanthiNessuna valutazione finora
- Fraktur CollesDocumento18 pagineFraktur CollesBerliana Kurniawati Nur HudaNessuna valutazione finora
- Phary Ngeal Arch Muscular Contributions Skeletal Contributions NerveDocumento3 paginePhary Ngeal Arch Muscular Contributions Skeletal Contributions NerveAmirul Ashraf Bin ShukeriNessuna valutazione finora
- AdhesiolysisDocumento44 pagineAdhesiolysisLeofe CorregidorNessuna valutazione finora
- Lefort 1 OsteotomyDocumento36 pagineLefort 1 OsteotomyNidhi Jayan100% (2)
- Breast Recosntruction Flap ProcedureDocumento41 pagineBreast Recosntruction Flap ProceduredewiswahyuNessuna valutazione finora
- Simple MastectomyDocumento3 pagineSimple MastectomyCindy DayocNessuna valutazione finora
- Hipo HiperthyroidDocumento49 pagineHipo HiperthyroidMuhammad Bilal Bin AmirNessuna valutazione finora
- Parotid GlandDocumento21 pagineParotid GlandHerlangga Fadhillah Akbar100% (1)
- Penurunan KesadaranDocumento52 paginePenurunan KesadaranEza MelindaNessuna valutazione finora
- Advanced SuturingDocumento18 pagineAdvanced SuturingAriyanie NurtaniaNessuna valutazione finora
- Kabwe Central Hospital KCH: Breast Cancer"Documento34 pagineKabwe Central Hospital KCH: Breast Cancer"Emmanuel MukukaNessuna valutazione finora
- Salivary Gland TumorDocumento62 pagineSalivary Gland Tumordeepak kumarNessuna valutazione finora
- CA MammaeDocumento30 pagineCA MammaeAlfiany SahrNessuna valutazione finora
- Journal ReadingDocumento14 pagineJournal ReadingCastiglianoNessuna valutazione finora
- Buttonhole DislocationDocumento13 pagineButtonhole DislocationHanif Andhika WardhanaNessuna valutazione finora
- Radical Neck Dissection: (RND) Classification, Indication and TechniquesDocumento42 pagineRadical Neck Dissection: (RND) Classification, Indication and TechniquesPatrycyaNessuna valutazione finora
- WIFI Score For Diabetes Foot UlcerDocumento17 pagineWIFI Score For Diabetes Foot Ulcertonylee24100% (1)
- BPHDocumento10 pagineBPHMichelle SalimNessuna valutazione finora
- Thyroid and Parathyroid GlandsDocumento5 pagineThyroid and Parathyroid GlandsChristopher PhilipsNessuna valutazione finora
- BS ParatiroidDocumento21 pagineBS ParatiroidNo StradamusNessuna valutazione finora
- Corona VariantsDocumento13 pagineCorona VariantsSajid NadafNessuna valutazione finora
- Severe COVID-19 LECTURE - Harvard 2021Documento49 pagineSevere COVID-19 LECTURE - Harvard 2021Sajid NadafNessuna valutazione finora
- Induction Agents: Don Daniels, M.DDocumento25 pagineInduction Agents: Don Daniels, M.DSajid NadafNessuna valutazione finora
- Transport of Oxygen and Carbon DioxideDocumento22 pagineTransport of Oxygen and Carbon DioxideSajid Nadaf100% (1)
- Anatomy of Musculoskeletal SystemDocumento6 pagineAnatomy of Musculoskeletal SystemSajid NadafNessuna valutazione finora
- Clinical Applications of Induced Hypothermia: Mark Luscombe John C AndrzejowskiDocumento5 pagineClinical Applications of Induced Hypothermia: Mark Luscombe John C AndrzejowskiSajid NadafNessuna valutazione finora
- Anaesthetic Record: Allergies Medications EscortDocumento1 paginaAnaesthetic Record: Allergies Medications EscortSajid NadafNessuna valutazione finora
- 2nd Lang EnglishDocumento23 pagine2nd Lang EnglishSajid NadafNessuna valutazione finora
- Chapter 4: Tissues, Part 1: Tissue A Collection of Cells That Perform RelatedDocumento23 pagineChapter 4: Tissues, Part 1: Tissue A Collection of Cells That Perform RelatedSajid NadafNessuna valutazione finora
- Chapter 4, Tissues, Part 2: Histology The Study of Tissues Tissue A Collection of Cells That Perform RelatedDocumento31 pagineChapter 4, Tissues, Part 2: Histology The Study of Tissues Tissue A Collection of Cells That Perform RelatedSajid NadafNessuna valutazione finora
- Cesarean Sections, Perfecting The Technique and Standardizing The Practice: An Analysis of The Book Obstetrícia, by Jorge de RezendeDocumento19 pagineCesarean Sections, Perfecting The Technique and Standardizing The Practice: An Analysis of The Book Obstetrícia, by Jorge de RezendeSajid NadafNessuna valutazione finora
- Visiting Time Morning 10.30 AM To 12.30 PM Afternoon 3.00 PM To 5.00 PMDocumento2 pagineVisiting Time Morning 10.30 AM To 12.30 PM Afternoon 3.00 PM To 5.00 PMSajid NadafNessuna valutazione finora
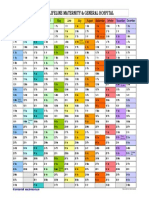
- 2018 Calendar Landscape in ColorDocumento1 pagina2018 Calendar Landscape in ColorSajid NadafNessuna valutazione finora
- Only 2 AttendersDocumento1 paginaOnly 2 AttendersSajid NadafNessuna valutazione finora
- Solar Water & Bathroom Provided Is Only For: Patient & BabiesDocumento2 pagineSolar Water & Bathroom Provided Is Only For: Patient & BabiesSajid NadafNessuna valutazione finora
- Arteria Temporal SuperficialDocumento6 pagineArteria Temporal SuperficialVictor Manuel Orozco VegaNessuna valutazione finora
- Sensation and Perception 9th Edition Goldstein Test BankDocumento10 pagineSensation and Perception 9th Edition Goldstein Test Bankgiaoagnesq3t100% (23)
- Case Epidural HematomaDocumento16 pagineCase Epidural HematomaBahRunNessuna valutazione finora
- Temporal Bone Dissection Dr. Stelian LUPESCUDocumento29 pagineTemporal Bone Dissection Dr. Stelian LUPESCUEdy MorarNessuna valutazione finora
- LarynxDocumento5 pagineLarynxGeraldine Marie SalvoNessuna valutazione finora
- ANP1106 ASyllabus 2020Documento5 pagineANP1106 ASyllabus 2020유우솔Nessuna valutazione finora
- Q2 G3 Science M1Documento40 pagineQ2 G3 Science M1Maricar AtienzaNessuna valutazione finora
- Orthodontic Aspects of Orthognathic Surgery - Shiva ShankarDocumento57 pagineOrthodontic Aspects of Orthognathic Surgery - Shiva Shankarnevin santhosh100% (1)
- Lecture Assignment # 5: Applied Anatomy of The Nervous SystemDocumento3 pagineLecture Assignment # 5: Applied Anatomy of The Nervous Systemjanela mae d. nabosNessuna valutazione finora
- Ectodermal Derivatives of Pig EmbryoDocumento7 pagineEctodermal Derivatives of Pig EmbryoChristalie Bea FernandezNessuna valutazione finora
- Medial MaxillectomyDocumento12 pagineMedial MaxillectomyJamesNessuna valutazione finora
- Algoritmo para El Tto Defectos NasalesDocumento14 pagineAlgoritmo para El Tto Defectos NasalesNicolás Silva GalvisNessuna valutazione finora
- 11 Nasal Cavity and Paranasal Sinuses-Dr - GosaiDocumento41 pagine11 Nasal Cavity and Paranasal Sinuses-Dr - GosaiDr.B.B.GosaiNessuna valutazione finora
- Hemifacial Microsomia: Presented by NithishDocumento29 pagineHemifacial Microsomia: Presented by NithishNithish ReddyNessuna valutazione finora
- Science Q2-Parts and Functions of The EyesDocumento31 pagineScience Q2-Parts and Functions of The EyesRovi ChellNessuna valutazione finora
- Lesson Plan 1Documento4 pagineLesson Plan 1api-383086643Nessuna valutazione finora
- Sleep Apnea SlidesDocumento49 pagineSleep Apnea SlidesGregory SNessuna valutazione finora
- 4b. Bimbingan Neuroimaging CT Scan Kepala 2 - ResidenDocumento60 pagine4b. Bimbingan Neuroimaging CT Scan Kepala 2 - ResidenDebby SejahteraNessuna valutazione finora
- Functional Neuroanatomy and Clinical Neuroscience - Foundations For Understanding Disorders of Cognition and Behavior 2022Documento465 pagineFunctional Neuroanatomy and Clinical Neuroscience - Foundations For Understanding Disorders of Cognition and Behavior 2022Eduardo RodriguezNessuna valutazione finora
- Special SensesDocumento21 pagineSpecial SensesZeeshan JalilNessuna valutazione finora
- Neurological AssessmentDocumento1 paginaNeurological AssessmentPrincess OycoNessuna valutazione finora
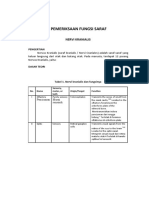
- Pemeriksaan Fungsi Saraf: Nervi KranialisDocumento14 paginePemeriksaan Fungsi Saraf: Nervi KranialisAfafa Win’sNessuna valutazione finora
- Cranial Nerves NeuroanatomyDocumento57 pagineCranial Nerves NeuroanatomyArvin TanNessuna valutazione finora
- Appearance VocabularyDocumento2 pagineAppearance VocabularyagaNessuna valutazione finora
- Neuroanatomy Text and Atlas - John D. Martin Copy-1Documento543 pagineNeuroanatomy Text and Atlas - John D. Martin Copy-1Francineide Freitas100% (1)
- Modern Dental Assisting 11Th Edition Bird Test Bank Full Chapter PDFDocumento37 pagineModern Dental Assisting 11Th Edition Bird Test Bank Full Chapter PDFRichardThompsonpcbd100% (9)
- Intranet.tdmu.Edu.ua Data Kafedra Internal Stomat Hir Classes Stud en Stomat Стоматология Ptn Хирургическая Стоматология 5 10 Semestr 25. Phlegmons of Submandibular, Submental Areas.htmDocumento1 paginaIntranet.tdmu.Edu.ua Data Kafedra Internal Stomat Hir Classes Stud en Stomat Стоматология Ptn Хирургическая Стоматология 5 10 Semestr 25. Phlegmons of Submandibular, Submental Areas.htmTri Sakti Sunda RomdhoniNessuna valutazione finora
- Unit II: Endocrine Nursing: Muhammad Yaqoob Instructor Ion-DuhsDocumento51 pagineUnit II: Endocrine Nursing: Muhammad Yaqoob Instructor Ion-DuhsyaqoobmdNessuna valutazione finora
- Head and Neck Block HandbookDocumento50 pagineHead and Neck Block HandbookGrace Poon OnionNessuna valutazione finora
- Nolte's The Human Brain An Introduction To Its Functional AnatomyDocumento658 pagineNolte's The Human Brain An Introduction To Its Functional AnatomyFausto Cruz100% (7)