Potrebbero piacerti anche
- Suspension Mansons 2Documento45 pagineSuspension Mansons 2Andres Silva67% (3)
- Mother To Child Transmission HBVDocumento48 pagineMother To Child Transmission HBVMuhammad FaisalNessuna valutazione finora
- ILRT Dr. Sarbani-1 PDFDocumento48 pagineILRT Dr. Sarbani-1 PDFdurgesh kumar100% (1)
- National AIDS Control Programme: Debajani NayakDocumento66 pagineNational AIDS Control Programme: Debajani NayakGandimareiNessuna valutazione finora
- Pediatric Hiv - Zambia.Documento59 paginePediatric Hiv - Zambia.Linus PuleNessuna valutazione finora
- Hepatitis B in Pregnancy PDFDocumento38 pagineHepatitis B in Pregnancy PDFAlsyNessuna valutazione finora
- Hiv Conference 2019Documento45 pagineHiv Conference 2019Keletso NyathiNessuna valutazione finora
- Population PyramidDocumento1 paginaPopulation PyramidBALOGO TRISHA MARIENessuna valutazione finora
- GPH Tutok Gamutan Davao OrientalDocumento3 pagineGPH Tutok Gamutan Davao Orientalrizza RiveraNessuna valutazione finora
- Use of Z-Scores For The Classification of MalnutritionDocumento16 pagineUse of Z-Scores For The Classification of Malnutritionapi-381899667% (3)
- Cancer and Risk of COVID-19 Through A General Community SurveyDocumento4 pagineCancer and Risk of COVID-19 Through A General Community SurveySimona VisanNessuna valutazione finora
- FindingsDocumento4 pagineFindingsAFRIZAL SHAHRIL MISRINessuna valutazione finora
- Mathematics School Based AssessmentDocumento12 pagineMathematics School Based AssessmentKatrina RampersadNessuna valutazione finora
- HTN Slide Deck NewDocumento27 pagineHTN Slide Deck NewChristy BerryNessuna valutazione finora
- Breakfast Intake Among Children and Adolescents: United States, 2015-2018Documento8 pagineBreakfast Intake Among Children and Adolescents: United States, 2015-2018Ánh NguyễnNessuna valutazione finora
- Ferrè Et Al.Documento19 pagineFerrè Et Al.martinsmicaelribeiroNessuna valutazione finora
- Tata Laksana Diabetes TerpaduDocumento74 pagineTata Laksana Diabetes TerpaduNovita Cahya PuspitasariNessuna valutazione finora
- Data Analysis CIA - 1Documento6 pagineData Analysis CIA - 1Albert Davis 2027916Nessuna valutazione finora
- 1-3 Day 1 - Community As People Community Health NursingDocumento11 pagine1-3 Day 1 - Community As People Community Health NursingBea Dela CenaNessuna valutazione finora
- Colorectal Cancer Screening in Alberta ...Documento23 pagineColorectal Cancer Screening in Alberta ...cydolusNessuna valutazione finora
- (FINAL) Prof. Dr. Dr. Bambang Budi Siswanto, SPJP (K) - Understanding HF in IndonesiaDocumento32 pagine(FINAL) Prof. Dr. Dr. Bambang Budi Siswanto, SPJP (K) - Understanding HF in IndonesiaTicksNessuna valutazione finora
- PN PDFDocumento59 paginePN PDFAmit PatelNessuna valutazione finora
- WHO-webinar Innovation Malaria EliminationDocumento20 pagineWHO-webinar Innovation Malaria EliminationAJ JaelaniNessuna valutazione finora
- Standar EtikDocumento13 pagineStandar Etikmuhammad bagusNessuna valutazione finora
- Final Slides Presentation .Documento49 pagineFinal Slides Presentation .Sanjida AhmedNessuna valutazione finora
- Health and Nutritional Status of Filipino Adults, 20-59 Years OldDocumento32 pagineHealth and Nutritional Status of Filipino Adults, 20-59 Years OldJose Mari TrinidadNessuna valutazione finora
- Prediabetes - (Slide For Speaker)Documento51 paginePrediabetes - (Slide For Speaker)Maya Sari HalimNessuna valutazione finora
- Diabetes Patient EducationDocumento96 pagineDiabetes Patient EducationbajaocNessuna valutazione finora
- HepB BD Experiences-Final - GhanaDocumento10 pagineHepB BD Experiences-Final - GhanaadhikatamaNessuna valutazione finora
- Gambaran Epid HIV IndonesiaDocumento32 pagineGambaran Epid HIV IndonesiaIsti'anah SururyNessuna valutazione finora
- Report COVID Clinical ManagmentDocumento70 pagineReport COVID Clinical ManagmentJeevan Emmanual JoyNessuna valutazione finora
- Program2 THN 2016Documento32 pagineProgram2 THN 2016leonardoNessuna valutazione finora
- Expanded National Nutrition Survey: 2019 Results: Health and Nutritional Status of Filipino Adults, 20-59 Years OldDocumento61 pagineExpanded National Nutrition Survey: 2019 Results: Health and Nutritional Status of Filipino Adults, 20-59 Years Oldzvfvr95hrkNessuna valutazione finora
- Smoking Adults PDFDocumento22 pagineSmoking Adults PDFJermeLou BaoNessuna valutazione finora
- Seminar Epidemi HIV Indonesia - 10april2019 - C6Documento59 pagineSeminar Epidemi HIV Indonesia - 10april2019 - C6Eny VeronikaNessuna valutazione finora
- SchoolidDocumento27 pagineSchoolidapi-392364749Nessuna valutazione finora
- Cohort Survival (S.Y. 2015 - 2016 To 2018 - 2019)Documento7 pagineCohort Survival (S.Y. 2015 - 2016 To 2018 - 2019)Mae LaglivaNessuna valutazione finora
- Group A PulsesDocumento30 pagineGroup A PulsesShravan N.V.Nessuna valutazione finora
- Afghanistan - Education Equity Profile For Adolescent GirlsDocumento16 pagineAfghanistan - Education Equity Profile For Adolescent GirlssalamNessuna valutazione finora
- Determinants SAARCDocumento24 pagineDeterminants SAARCmititelualex1Nessuna valutazione finora
- Research DesignedDocumento14 pagineResearch DesignedAsad HussainNessuna valutazione finora
- UTS PraktikumEkonometrika Nadia Rachmani Putri - ES2 - 204105020056Documento9 pagineUTS PraktikumEkonometrika Nadia Rachmani Putri - ES2 - 204105020056Nadia Rahmani PutriNessuna valutazione finora
- Child Nutrition: Darmono SSDocumento53 pagineChild Nutrition: Darmono SSKiky SuryaNessuna valutazione finora
- National 2010 RAPID-Presidential Term PDFDocumento41 pagineNational 2010 RAPID-Presidential Term PDFLeyrra Paclibar DiduloNessuna valutazione finora
- SABSSM FINAL LAUNCH Presentation 27november2023 1Documento32 pagineSABSSM FINAL LAUNCH Presentation 27november2023 1Princess MahogoNessuna valutazione finora
- 11 - Presenting Quantitative Data ResultsDocumento8 pagine11 - Presenting Quantitative Data ResultsNguyen Nguy noenNessuna valutazione finora
- Madronio-Bsee2c-Activity 2.1Documento3 pagineMadronio-Bsee2c-Activity 2.1Mark Stephen MadronioNessuna valutazione finora
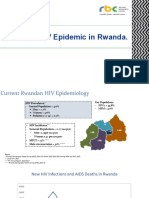
- State of HIV Epidemic in RwandaDocumento17 pagineState of HIV Epidemic in RwandaNshimiyimana Jean ClaudeNessuna valutazione finora
- The Barbados Drug Information Network: Findings From The 2017 & 2018 ReportsDocumento49 pagineThe Barbados Drug Information Network: Findings From The 2017 & 2018 Reportsterrod gangstaNessuna valutazione finora
- Adolescent TuberculosisDocumento29 pagineAdolescent TuberculosistioNessuna valutazione finora
- MediCall - Nursing Informatics App Proposal PDFDocumento20 pagineMediCall - Nursing Informatics App Proposal PDFPaul MarloweNessuna valutazione finora
- Degree Outcomes Statement 2022Documento11 pagineDegree Outcomes Statement 2022AubreyNessuna valutazione finora
- Acute Viral HepatitisDocumento76 pagineAcute Viral HepatitisSaurabh SagunNessuna valutazione finora
- No Program Indikator Kinerja Ukm Sasaran Capaian % Sasaran Capaian % Promosi Kesehatan Target 2018 Target 2017Documento9 pagineNo Program Indikator Kinerja Ukm Sasaran Capaian % Sasaran Capaian % Promosi Kesehatan Target 2018 Target 2017susiNessuna valutazione finora
- 1 - Longer Term Tolerability and Efficacy of Zyn002 Cannabidiol Transderm)Documento10 pagine1 - Longer Term Tolerability and Efficacy of Zyn002 Cannabidiol Transderm)Esraa SaeedNessuna valutazione finora
- Opening of Classess Keytodac Cs 2022Documento15 pagineOpening of Classess Keytodac Cs 2022Paaralang Sentral Ng KeytodacNessuna valutazione finora
- Antihistamines in The Treatment of Pruritus in Psoriasis: Original PaperDocumento7 pagineAntihistamines in The Treatment of Pruritus in Psoriasis: Original PapersakelengelNessuna valutazione finora
- Midas Safety - NFO PresentationDocumento12 pagineMidas Safety - NFO PresentationAbbas NaqviNessuna valutazione finora
- The Preliminary Findings of South Africa's Latest HIV Household SurveyDocumento4 pagineThe Preliminary Findings of South Africa's Latest HIV Household SurveyBhekisisa HealthNessuna valutazione finora
- RAW TM & HM Users Manual V 11Documento8 pagineRAW TM & HM Users Manual V 11arcangelus22Nessuna valutazione finora
- Hibike Euphonium - Crescent Moon DanceDocumento22 pagineHibike Euphonium - Crescent Moon Dancelezhi zhangNessuna valutazione finora
- ReferencesDocumento12 pagineReferencesBilal RazzaqNessuna valutazione finora
- EY Global Hospitality Insights 2016Documento24 pagineEY Global Hospitality Insights 2016Anonymous BkmsKXzwyKNessuna valutazione finora
- PCU 200 Handbook 2018-19 PDFDocumento177 paginePCU 200 Handbook 2018-19 PDFVica CapatinaNessuna valutazione finora
- RRLDocumento4 pagineRRLElaine Lacandula100% (1)
- Oblicon NotesDocumento14 pagineOblicon NotesCee Silo Aban100% (1)
- Syllabus Spring 2021Documento17 pagineSyllabus Spring 2021Eden ParkNessuna valutazione finora
- Trading SecretsDocumento99 pagineTrading SecretsGary100% (3)
- Gremath Set8-1Documento48 pagineGremath Set8-1uzairmetallurgistNessuna valutazione finora
- Auto Loan Application Form - IndividualDocumento2 pagineAuto Loan Application Form - IndividualKlarise EspinosaNessuna valutazione finora
- KGTE February 2011 ResultDocumento60 pagineKGTE February 2011 ResultSupriya NairNessuna valutazione finora
- Polymer ConcreteDocumento15 paginePolymer ConcreteHew LockNessuna valutazione finora
- BI410 Plant Developmental BiologyDocumento41 pagineBI410 Plant Developmental BiologyLaisla CagliariNessuna valutazione finora
- Industrial Thread (Sewing Thread)Documento8 pagineIndustrial Thread (Sewing Thread)sandhyaishtaNessuna valutazione finora
- Jacksonville's Taste 2012Documento100 pagineJacksonville's Taste 2012Ali KhanNessuna valutazione finora
- Revilla Law IRRDocumento2 pagineRevilla Law IRRPaulNessuna valutazione finora
- Tesla, Inc.: Jump To Navigation Jump To Search Tesla Induction Motor AC MotorDocumento90 pagineTesla, Inc.: Jump To Navigation Jump To Search Tesla Induction Motor AC MotorEdi RaduNessuna valutazione finora
- National Golf Club FactsheetDocumento24 pagineNational Golf Club FactsheetCris MefNessuna valutazione finora
- Revalida ResearchDocumento3 pagineRevalida ResearchJakie UbinaNessuna valutazione finora
- BZU Ad 31 12 12Documento15 pagineBZU Ad 31 12 12Saleem MirraniNessuna valutazione finora
- Rubrics On Video Analysis - 2022Documento2 pagineRubrics On Video Analysis - 2022jovenil BacatanNessuna valutazione finora
- Teaching Students With High Incidence Disabilities Strategies For Diverse Classrooms 1St Edition Prater Test Bank Full Chapter PDFDocumento35 pagineTeaching Students With High Incidence Disabilities Strategies For Diverse Classrooms 1St Edition Prater Test Bank Full Chapter PDFvaleriewashingtonfsnxgzyjbi100% (6)
- Scrabble Scrabble Is A Word Game in Which Two or Four Players Score Points by Placing Tiles, EachDocumento4 pagineScrabble Scrabble Is A Word Game in Which Two or Four Players Score Points by Placing Tiles, EachNathalie Faye De PeraltaNessuna valutazione finora
- Cambridge IGCSE: PHYSICS 0625/63Documento16 pagineCambridge IGCSE: PHYSICS 0625/63...Nessuna valutazione finora
- Warcraft III ManualDocumento47 pagineWarcraft III Manualtrevorbourget78486100% (6)
- US. Peace Corps Tetun Language CourseDocumento305 pagineUS. Peace Corps Tetun Language CoursePeter W Gossner100% (1)
- 2202 Infantilization Essay - Quinn WilsonDocumento11 pagine2202 Infantilization Essay - Quinn Wilsonapi-283151250Nessuna valutazione finora
- UCCP Magna Carta For Church WorkersDocumento39 pagineUCCP Magna Carta For Church WorkersSilliman Ministry Magazine83% (12)