Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Mathematics 2016-January P1 PDFDocumento9 pagineMathematics 2016-January P1 PDFMichael TimsonNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Prose 2020Documento27 pagineProse 2020Danielle Johns50% (2)
- Math2008 PDFDocumento11 pagineMath2008 PDFDanielle JohnsNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- ReflexesDocumento29 pagineReflexesWawan AryawanNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Personal Monthly Budget 1Documento1 paginaPersonal Monthly Budget 1Anees SulaimanNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Personal Monthly Budget 1Documento1 paginaPersonal Monthly Budget 1Anees SulaimanNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Pharmacology - Cardiovascular SystemDocumento98 paginePharmacology - Cardiovascular SystemDanielle JohnsNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- CommunicationDocumento52 pagineCommunicationDanielle JohnsNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Personal Monthly Budget 1Documento1 paginaPersonal Monthly Budget 1Anees SulaimanNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
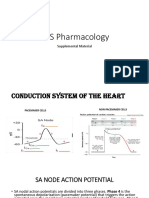
- CVS Pharmacology Supplemental SlidesDocumento7 pagineCVS Pharmacology Supplemental SlidesDanielle JohnsNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Negatives and ApocopationDocumento13 pagineNegatives and ApocopationDanielle JohnsNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Csec English B p02 May 2017 PDFDocumento28 pagineCsec English B p02 May 2017 PDFShantel MyersNessuna valutazione finora
- Characters in The TempestDocumento3 pagineCharacters in The TempestDanielle JohnsNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- IndirectdirectbydaniDocumento23 pagineIndirectdirectbydaniDanielle JohnsNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Uses of Static ElectricityDocumento11 pagineUses of Static ElectricityDanielle JohnsNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Pediatric LeukemiasDocumento42 paginePediatric LeukemiasslyfoxkittyNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Equipos Monitoreo de CondicionesDocumento11 pagineEquipos Monitoreo de CondicionesJonathan Vasquez LlagunoNessuna valutazione finora
- (FEU) Central Venous Pressure Notes PDFDocumento25 pagine(FEU) Central Venous Pressure Notes PDFBryJos tiongsonNessuna valutazione finora
- Naloxone (Narcan)Documento2 pagineNaloxone (Narcan)Adrianne BazoNessuna valutazione finora
- 8 - Sullivan - Interpersonal TheoryDocumento4 pagine8 - Sullivan - Interpersonal TheorystephanieNessuna valutazione finora
- Approach To A Patient With Upper GI BleedDocumento42 pagineApproach To A Patient With Upper GI BleedMuhammad Naveed AslamNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Tinea Cruris Abq JournalDocumento3 pagineTinea Cruris Abq JournalGustiandari FidhyaNessuna valutazione finora
- Classification and Patient Selection in Abdominoplasty: Alan Matarasso, MD, FacsDocumento8 pagineClassification and Patient Selection in Abdominoplasty: Alan Matarasso, MD, FacsPopa FlorinNessuna valutazione finora
- Buset Na ResearchDocumento5 pagineBuset Na Researchmk soberanoNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Sharma Et Al-2016-Journal of Applied MicrobiologyDocumento11 pagineSharma Et Al-2016-Journal of Applied MicrobiologyJoanaNessuna valutazione finora
- Essentials of Orthognathic Surgery, 3eDocumento14 pagineEssentials of Orthognathic Surgery, 3epaolacsuarezaNessuna valutazione finora
- 30 - Gag Reflex - Causes and ManagementDocumento4 pagine30 - Gag Reflex - Causes and ManagementNadiyah Rizqi ANessuna valutazione finora
- Abdomenul AcutDocumento5 pagineAbdomenul Acutcristina ovidenieNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (120)
- Lecture 2Documento4 pagineLecture 2Peter KiptumNessuna valutazione finora
- Cae Open Cloze PhobiasDocumento3 pagineCae Open Cloze PhobiasValéria DuczaNessuna valutazione finora
- NCPDocumento1 paginaNCPVictor MurilloNessuna valutazione finora
- Combination of Angkak (Red Yeast Rice), Red Guava (Psidium Guajava Linn) Leaf Extract and Red Guava Fruit Juice Increase Thrombocyte in Quinine-Exposed RatsDocumento6 pagineCombination of Angkak (Red Yeast Rice), Red Guava (Psidium Guajava Linn) Leaf Extract and Red Guava Fruit Juice Increase Thrombocyte in Quinine-Exposed RatsIOSR Journal of PharmacyNessuna valutazione finora
- A Critical Review of Swarnaprashan As A BoonDocumento24 pagineA Critical Review of Swarnaprashan As A BoonRashmi SharmaNessuna valutazione finora
- Antiaritmice Clasa I A MedicamentDocumento3 pagineAntiaritmice Clasa I A MedicamentAndreea ElenaNessuna valutazione finora
- Tesis vITAMIN C CONTENT IN FRUITSDocumento24 pagineTesis vITAMIN C CONTENT IN FRUITSHema JothyNessuna valutazione finora
- Marketing Sensing FrameworkDocumento8 pagineMarketing Sensing FrameworkHaseeb Ali0% (1)
- K6 - Tetanus PEDIATRICDocumento23 pagineK6 - Tetanus PEDIATRICbanuperiahNessuna valutazione finora
- ScabiesDocumento5 pagineScabiespakemainmainNessuna valutazione finora
- Pelvic Inflammatory DiseaseDocumento34 paginePelvic Inflammatory DiseaseOhunakin AfolabiNessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Seminar Molar DistalizationDocumento130 pagineSeminar Molar DistalizationMuhsina EyyanathilNessuna valutazione finora
- SBRT PDFDocumento14 pagineSBRT PDFrubenNessuna valutazione finora
- The Information About EDSDocumento3 pagineThe Information About EDSAmber100% (1)
- Ehz 467Documento65 pagineEhz 467Coy Calapatia-TorresNessuna valutazione finora
- Diseases of The Hair and ScalpDocumento7 pagineDiseases of The Hair and Scalprl20Nessuna valutazione finora
- CPD Questions For Volume 21 Issue 3Documento4 pagineCPD Questions For Volume 21 Issue 3KeeranmayeeishraNessuna valutazione finora