Potrebbero piacerti anche
- Self Assessment in Musculoskeletal Pathology X-raysDa EverandSelf Assessment in Musculoskeletal Pathology X-raysValutazione: 5 su 5 stelle5/5 (2)
- Fast Spin Echo: Bioe 594 - Advanced Topics in Mri Nick GruszauskasDocumento42 pagineFast Spin Echo: Bioe 594 - Advanced Topics in Mri Nick GruszauskasagithiaNessuna valutazione finora
- Basic Pulse SequencesDocumento10 pagineBasic Pulse Sequencesjunghs2000Nessuna valutazione finora
- Radiology Quiz Workbook for Medical StudentsDocumento11 pagineRadiology Quiz Workbook for Medical StudentsMădălina CiobotariuNessuna valutazione finora
- Ficat and Arlet staging of hip AVNDocumento6 pagineFicat and Arlet staging of hip AVNFernando Sugiarto0% (1)
- Cervical Spine Trauma Imaging GuideDocumento25 pagineCervical Spine Trauma Imaging GuideComagaNessuna valutazione finora
- Musculoskeletal Imaging 2015Documento79 pagineMusculoskeletal Imaging 2015Faiq Syukri Bin SaparudinNessuna valutazione finora
- MRI Bioeffects and SafetyDocumento54 pagineMRI Bioeffects and SafetyYuda FhunkshyangNessuna valutazione finora
- Balancing TKADocumento9 pagineBalancing TKAMuhammad Tabish SaleemNessuna valutazione finora
- Summary of BASICS OF DIFFUSION MRI PDFDocumento13 pagineSummary of BASICS OF DIFFUSION MRI PDFParamitha AdriyatiNessuna valutazione finora
- Basic Principles of Radiology: Bachtiar MurtalaDocumento75 pagineBasic Principles of Radiology: Bachtiar MurtalaMargaretha SonoNessuna valutazione finora
- Skeletal Radiology Interpretation GuideDocumento89 pagineSkeletal Radiology Interpretation GuideRivani KurniawanNessuna valutazione finora
- Diagnostic Radiology MCQ ReviewDocumento7 pagineDiagnostic Radiology MCQ ReviewMuhammad TariqNessuna valutazione finora
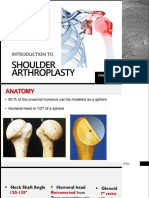
- KHA Shoulder Arthroplasty FinalDocumento27 pagineKHA Shoulder Arthroplasty FinalKyaw Htet Aung100% (1)
- Six Minute Walk Test - : Nimisha B (MPT, Dyhe) Assisstant Professor Sacpms, MMC ModakkallurDocumento16 pagineSix Minute Walk Test - : Nimisha B (MPT, Dyhe) Assisstant Professor Sacpms, MMC ModakkallurNimisha Balakrishnan100% (1)
- Interpretation of Bone and Joint RadiographyDocumento68 pagineInterpretation of Bone and Joint RadiographyBadrul MunirNessuna valutazione finora
- Avascular NecrosisDocumento3 pagineAvascular Necrosisahmad shaltoutNessuna valutazione finora
- Acetabular FractureDocumento37 pagineAcetabular FractureSandeep Gurung Nepali100% (1)
- Sectra-The Radiologists Handbook For Future Excellence 2020Documento30 pagineSectra-The Radiologists Handbook For Future Excellence 2020Xhenni Xhenni100% (1)
- UKA: When Would I Do It?Documento35 pagineUKA: When Would I Do It?neareastspineNessuna valutazione finora
- Intra Oral Radiography: - Presented byDocumento34 pagineIntra Oral Radiography: - Presented byNehal MainaliNessuna valutazione finora
- Spinal TumorsDocumento59 pagineSpinal TumorsAl-Banji MohammadNessuna valutazione finora
- CVM6101 Anatomy SpineDocumento7 pagineCVM6101 Anatomy SpineHéctor LópezNessuna valutazione finora
- Radiography of Forearm and Upper ArmDocumento35 pagineRadiography of Forearm and Upper ArmsaurabhmhshwrNessuna valutazione finora
- G03-Vascular InjuryDocumento47 pagineG03-Vascular InjurySatrio Bangun Negoro100% (1)
- Aaos PDFDocumento4 pagineAaos PDFWisnu CahyoNessuna valutazione finora
- Bankurt RadiologyDocumento22 pagineBankurt RadiologyVajja SwatiNessuna valutazione finora
- Giant Cell TumourDocumento61 pagineGiant Cell Tumourvictormoirangthem100% (1)
- Visualize GI Tract Abnormalities with Barium StudyDocumento34 pagineVisualize GI Tract Abnormalities with Barium StudyJahanavi JaluNessuna valutazione finora
- Mri Master RodillaDocumento9 pagineMri Master RodillaAndrea BelénNessuna valutazione finora
- Tendon TransferDocumento1 paginaTendon TransferPandi Smart VjNessuna valutazione finora
- Lumber Spine and Pelvis RadiographyDocumento84 pagineLumber Spine and Pelvis RadiographyMunish DograNessuna valutazione finora
- Skull RadiographyDocumento104 pagineSkull RadiographyEzra NserekoNessuna valutazione finora
- Master Radiology Notes GIT PDFDocumento115 pagineMaster Radiology Notes GIT PDFuroshkgNessuna valutazione finora
- Rapid ReportingDocumento249 pagineRapid ReportingYuki NgNessuna valutazione finora
- Corticospinal Tract: Functions and Clinical RelevanceDocumento4 pagineCorticospinal Tract: Functions and Clinical RelevanceNrs Sani Sule MashiNessuna valutazione finora
- Bones Anatomy: Wiki RadiographyDocumento59 pagineBones Anatomy: Wiki RadiographyniputusellyowNessuna valutazione finora
- Introduction To Orthopedic ImagingDocumento72 pagineIntroduction To Orthopedic ImagingNovien WilindaNessuna valutazione finora
- MRI Protocols GuideDocumento5 pagineMRI Protocols Guidealvi5nNessuna valutazione finora
- 1.26 (Surgery) Orthopedic Pathology - OncologyDocumento7 pagine1.26 (Surgery) Orthopedic Pathology - OncologyLeo Mari Go LimNessuna valutazione finora
- Film Critique of The Upper Extremity - Part 1 - Shoulder, Clavicle, and HumerusDocumento77 pagineFilm Critique of The Upper Extremity - Part 1 - Shoulder, Clavicle, and Humerussadbad6Nessuna valutazione finora
- Clinical Uses and Technical Advances of Diffusion MRIDocumento13 pagineClinical Uses and Technical Advances of Diffusion MRICristian Martinez BocazNessuna valutazione finora
- Bone Resorption and Deposition in OrthopaedicsDocumento2 pagineBone Resorption and Deposition in OrthopaedicsAnna SeeNessuna valutazione finora
- Bone AgeDocumento65 pagineBone AgeueumanaNessuna valutazione finora
- Neoplasm On Bone and Soft Tissue MikoDocumento151 pagineNeoplasm On Bone and Soft Tissue Mikoindra muhammadNessuna valutazione finora
- Essential Guidelines for Trauma RadiographyDocumento69 pagineEssential Guidelines for Trauma RadiographySyuhada AzmiNessuna valutazione finora
- X-Ray Interpretation Skills: Dr. Hisham AlsanawiDocumento68 pagineX-Ray Interpretation Skills: Dr. Hisham AlsanawiVika DamayNessuna valutazione finora
- Aplication of MRI Contrast AgentDocumento26 pagineAplication of MRI Contrast AgentDKpaljrixNessuna valutazione finora
- MR Requirements Musculoskeletal MRIDocumento56 pagineMR Requirements Musculoskeletal MRIDifa ZafiraNessuna valutazione finora
- Radiography of The Thoracic SpineDocumento59 pagineRadiography of The Thoracic SpineEzra NserekoNessuna valutazione finora
- Spine TraumaDocumento52 pagineSpine Traumaapi-26159412100% (1)
- Basics of Chest X-Ray Interpretation (39Documento23 pagineBasics of Chest X-Ray Interpretation (39Rabi Dhakal100% (1)
- Skull XrayDocumento35 pagineSkull XrayWebster The-TechGuy LunguNessuna valutazione finora
- Pelvic Radiograph Views: Techniques and TechnicalitiesDocumento30 paginePelvic Radiograph Views: Techniques and TechnicalitiesGayle Grey100% (1)
- Mri Brain SequencesDocumento13 pagineMri Brain SequencesRisa MarissaNessuna valutazione finora
- Applied Surgical AnatomyDocumento52 pagineApplied Surgical AnatomyEmad AdelNessuna valutazione finora
- Bone TumorsDocumento29 pagineBone TumorsmatameaNessuna valutazione finora
- Knee MriDocumento32 pagineKnee MriSyahrul RaziNessuna valutazione finora
- ACL GraftDocumento10 pagineACL GraftWorthless BoysNessuna valutazione finora
- Jimed, Vol. 3, No. 2 Issn 2356-301XDocumento5 pagineJimed, Vol. 3, No. 2 Issn 2356-301XDewi YulyantiNessuna valutazione finora
- Spinal Cord Lesion Learning ModuleDocumento37 pagineSpinal Cord Lesion Learning Moduleเกมกวี MedicalStudentNessuna valutazione finora
- Intramedullary Lesions in NF1 and NF2 NXPowerLiteDocumento14 pagineIntramedullary Lesions in NF1 and NF2 NXPowerLiteWorthless BoysNessuna valutazione finora
- Metastatic Tumor of Spine-1Documento128 pagineMetastatic Tumor of Spine-1Worthless BoysNessuna valutazione finora
- Bajammal 2006 Spinal TumorsDocumento76 pagineBajammal 2006 Spinal TumorsWorthless BoysNessuna valutazione finora
- Wrist Mass.Documento1 paginaWrist Mass.Worthless BoysNessuna valutazione finora
- Spinal Cord Lesions GuideDocumento43 pagineSpinal Cord Lesions GuideWorthless Boys100% (4)
- Hemoragie CerebralaDocumento23 pagineHemoragie CerebralaClaudia MoldovanuNessuna valutazione finora
- Spinal Intramedullary Tubercular Abscess Case ReportDocumento4 pagineSpinal Intramedullary Tubercular Abscess Case ReportWorthless BoysNessuna valutazione finora
- Spinal Cord Tumors د.عارفDocumento43 pagineSpinal Cord Tumors د.عارفMohammad BelbahaithNessuna valutazione finora
- MRI Neonatal Brain PDFDocumento12 pagineMRI Neonatal Brain PDFWorthless BoysNessuna valutazione finora
- Brain Fungal InfectionDocumento14 pagineBrain Fungal InfectionWorthless BoysNessuna valutazione finora
- Neurovascular CompressionDocumento9 pagineNeurovascular CompressionWorthless BoysNessuna valutazione finora
- MRI PlanesDocumento25 pagineMRI PlanesCaroline HonNessuna valutazione finora
- ACL GraftDocumento10 pagineACL GraftWorthless BoysNessuna valutazione finora
- Duchenne Muscular Dystrophy: Causes, Symptoms & TreatmentsDocumento18 pagineDuchenne Muscular Dystrophy: Causes, Symptoms & TreatmentsLusi MunawarohNessuna valutazione finora
- Improving The Patient Experience Through Provider Communication S PDFDocumento6 pagineImproving The Patient Experience Through Provider Communication S PDFWagiono SuparanNessuna valutazione finora
- Procedure-for-taking-Blood-Culture - Feb-2015 PDFDocumento5 pagineProcedure-for-taking-Blood-Culture - Feb-2015 PDFVesna CucaNessuna valutazione finora
- Operative PDFDocumento126 pagineOperative PDFSimran Arora100% (1)
- Prehospital Trauma Care PDFDocumento6 paginePrehospital Trauma Care PDFU VenkateshNessuna valutazione finora
- Interprofessional Collaboration: Three Best Practice Models of Interprofessional EducationDocumento5 pagineInterprofessional Collaboration: Three Best Practice Models of Interprofessional Educationna5649Nessuna valutazione finora
- The Challenges of Effective Communication Between Health Information Officers and PatientsDocumento5 pagineThe Challenges of Effective Communication Between Health Information Officers and Patientshassan mamudNessuna valutazione finora
- GP Mental State Exam OSCEDocumento2 pagineGP Mental State Exam OSCEJagdishVankarNessuna valutazione finora
- Perio Notes CombinedDocumento71 paginePerio Notes CombinedHayley WelshNessuna valutazione finora
- The Back Book PDFDocumento14 pagineThe Back Book PDFfoldsnholdsNessuna valutazione finora
- Recommendation Letter - BeverlyDocumento2 pagineRecommendation Letter - Beverlyapi-355180754100% (2)
- The Influence of Angles Kappa and Alpha and Pupil Size On Vision After Implantation of Soleko Evolve and Lucidis Lenses With A Pure EDOF StructureDocumento12 pagineThe Influence of Angles Kappa and Alpha and Pupil Size On Vision After Implantation of Soleko Evolve and Lucidis Lenses With A Pure EDOF StructureAthenaeum Scientific PublishersNessuna valutazione finora
- Cpdprogram Pharmacy 82318Documento81 pagineCpdprogram Pharmacy 82318PRC BoardNessuna valutazione finora
- LTCW Breast Write UpDocumento21 pagineLTCW Breast Write Upapi-632682404Nessuna valutazione finora
- Crossword PuzzleDocumento2 pagineCrossword PuzzleJohn Patric Plaida100% (1)
- Death and DyingDocumento3 pagineDeath and DyingAlphonce GeorgeNessuna valutazione finora
- Argumentative Plastic SurgeryDocumento6 pagineArgumentative Plastic SurgeryMariell PenaroyoNessuna valutazione finora
- Delegation - ManagementDocumento8 pagineDelegation - ManagementDianne Ebro100% (1)
- History of NeuroscienceDocumento3 pagineHistory of Neurosciencemihaela irofteNessuna valutazione finora
- Perilymph FistulaDocumento4 paginePerilymph FistulavieeveeNessuna valutazione finora
- Nursing Practice I - Foundation of Professional NursingDocumento9 pagineNursing Practice I - Foundation of Professional NursingNeenya SisonNessuna valutazione finora
- Dengue Is Transmitted by The Bite of An Aedesmosquito Infected With Any One of The Four DengueDocumento6 pagineDengue Is Transmitted by The Bite of An Aedesmosquito Infected With Any One of The Four DengueKatrina PonceNessuna valutazione finora
- Inner Demon Destroyer MakeshiftDocumento18 pagineInner Demon Destroyer MakeshiftMike H100% (1)
- The Perfect TenDocumento10 pagineThe Perfect TenVágó GáborNessuna valutazione finora
- Cardio, Otis, Ortho, and GI Drug ListsDocumento4 pagineCardio, Otis, Ortho, and GI Drug ListsJodi Gugel DeMarrowNessuna valutazione finora
- Monografía de InglesDocumento17 pagineMonografía de InglesDavid SaucedoNessuna valutazione finora
- Legacy Participants and Legacy Applicants Fact Sheet: Who May Qualify For PCAFC?Documento3 pagineLegacy Participants and Legacy Applicants Fact Sheet: Who May Qualify For PCAFC?Cliff AkasNessuna valutazione finora
- Diversity Tool PDFDocumento3 pagineDiversity Tool PDFmr_jamzNessuna valutazione finora
- Aldactone SpironlactoneDocumento1 paginaAldactone SpironlactoneCassie100% (1)
- Reflection JournalDocumento28 pagineReflection JournalDeniz SalesNessuna valutazione finora