Potrebbero piacerti anche
- Determinant of Morbidity 2022Documento25 pagineDeterminant of Morbidity 2022Wilson HalimNessuna valutazione finora
- Lecture 1 CBP Topik 1Documento22 pagineLecture 1 CBP Topik 1citra suciptaNessuna valutazione finora
- 1 Determinant of MorbidityDocumento55 pagine1 Determinant of MorbidityGrace88 2016Nessuna valutazione finora
- Konsep Timbulnya Penyakit Dalam Pendekatan EpidemiologiDocumento21 pagineKonsep Timbulnya Penyakit Dalam Pendekatan EpidemiologiDyah AjengNessuna valutazione finora
- Konsep Timbulnya PenyakitDocumento21 pagineKonsep Timbulnya Penyakitfarrelbz1Nessuna valutazione finora
- Determinants of Health - RandhirDocumento35 pagineDeterminants of Health - RandhirRANDHIR DHAKANessuna valutazione finora
- Health and H BehaviorDocumento69 pagineHealth and H BehaviorDawud AsnakewNessuna valutazione finora
- Introtoepi 2022Documento47 pagineIntrotoepi 2022Kanwal KhanNessuna valutazione finora
- Epidemiologi Pa WandiDocumento57 pagineEpidemiologi Pa WandiWinardiNessuna valutazione finora
- Lesson 5 Epidemiology and Public Health For Med Students 2022-2023Documento62 pagineLesson 5 Epidemiology and Public Health For Med Students 2022-2023salemNessuna valutazione finora
- Concept of Disease: DR - Abdifatah Ahmed AbdullahiDocumento15 pagineConcept of Disease: DR - Abdifatah Ahmed AbdullahiSomali Medical StudentsNessuna valutazione finora
- Epidemiology in Community Health NursingDocumento25 pagineEpidemiology in Community Health NursingPornillosa, Jenaehl Mikhail S.Nessuna valutazione finora
- DR ShabirDocumento30 pagineDR Shabirjk045413Nessuna valutazione finora
- Epidemiological Approach: Prepared by I Gede Purnawinadi, S.Kep., NS., M.Kes., CWCCADocumento16 pagineEpidemiological Approach: Prepared by I Gede Purnawinadi, S.Kep., NS., M.Kes., CWCCAKathleen SharonNessuna valutazione finora
- Introduction To The Fundamentals of EpidemiologyDocumento29 pagineIntroduction To The Fundamentals of EpidemiologyakankshaNessuna valutazione finora
- Materi OH SMART - ToT 2017cinagaraDocumento133 pagineMateri OH SMART - ToT 2017cinagaraNura MashumahNessuna valutazione finora
- Costy Pandjaitan, SKM.,MARSDocumento49 pagineCosty Pandjaitan, SKM.,MARSsilviNessuna valutazione finora
- Public Health NotesDocumento25 paginePublic Health NotesletaplayapNessuna valutazione finora
- Null 5Documento62 pagineNull 5Esdras DountioNessuna valutazione finora
- Epidemiology: Dr. Siswanto, M.SCDocumento65 pagineEpidemiology: Dr. Siswanto, M.SCSharan SekhonNessuna valutazione finora
- Socio - Cultural and Ethnographic Research in Public HealthDocumento33 pagineSocio - Cultural and Ethnographic Research in Public Healthjencarr2Nessuna valutazione finora
- 2 Konsep Sehat Dan Determinan KesehatanDocumento50 pagine2 Konsep Sehat Dan Determinan KesehatanaditaNessuna valutazione finora
- Why Community Medicine?Documento54 pagineWhy Community Medicine?Saher ShahzadNessuna valutazione finora
- Lecture - Models of Health, Competing or Complementary Handout SlidesDocumento14 pagineLecture - Models of Health, Competing or Complementary Handout SlidesRajveen ChahalNessuna valutazione finora
- Natural History of DiseaseDocumento70 pagineNatural History of DiseasePalwasha Khan0% (1)
- Epidemiology - AK - FinalDocumento115 pagineEpidemiology - AK - FinalkarthikNessuna valutazione finora
- SDOHDocumento23 pagineSDOHNezer SorianoNessuna valutazione finora
- 1.pengantar IKM& Paradigma SehatDocumento19 pagine1.pengantar IKM& Paradigma SehatLucky fazriyaniNessuna valutazione finora
- By: Siti Pariani, DR, MS, MSC, PH.D Depart Public Health and Preventive Medicine School of Medicine, Airlangga UniversityDocumento17 pagineBy: Siti Pariani, DR, MS, MSC, PH.D Depart Public Health and Preventive Medicine School of Medicine, Airlangga UniversityIanMarvinGNessuna valutazione finora
- Basic Concepts and Principles of EpidemiologyDocumento22 pagineBasic Concepts and Principles of EpidemiologyCalingalan Hussin CaluangNessuna valutazione finora
- Theories in MortalityDocumento95 pagineTheories in MortalityTere MapiliNessuna valutazione finora
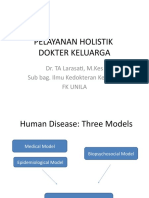
- Pelayanan Holistik Dokter Keluarga: Dr. TA Larasati, M.Kes Sub Bag. Ilmu Kedokteran Keluarga FK UnilaDocumento27 paginePelayanan Holistik Dokter Keluarga: Dr. TA Larasati, M.Kes Sub Bag. Ilmu Kedokteran Keluarga FK UnilaMutiara KhalishNessuna valutazione finora
- Hiap PPT Module 1 Part 2Documento16 pagineHiap PPT Module 1 Part 2Sree LathaNessuna valutazione finora
- B.SC II Yr CHN Epi Approach and Triad Part II 1Documento38 pagineB.SC II Yr CHN Epi Approach and Triad Part II 1NirmalaNessuna valutazione finora
- What Is EpidemiologyDocumento34 pagineWhat Is EpidemiologyFYMNessuna valutazione finora
- Introduction To The Fundamentals of Epidemiology: Thomas Songer, PHDDocumento36 pagineIntroduction To The Fundamentals of Epidemiology: Thomas Songer, PHDJamriKallunNessuna valutazione finora
- Concept of Health and Disease and PreventionDocumento57 pagineConcept of Health and Disease and PreventionPrabhu Aypa100% (2)
- PSM Lecture SeriesDocumento35 paginePSM Lecture SeriesCoy EnNessuna valutazione finora
- Dr. Farooq LectureDocumento30 pagineDr. Farooq LectureaqeelNessuna valutazione finora
- Epidemiological Triad and Other ModelsDocumento20 pagineEpidemiological Triad and Other ModelsSyed BuRhan Ud-DinNessuna valutazione finora
- Social Determinants of HealthDocumento44 pagineSocial Determinants of HealthAlaa Abu AishehNessuna valutazione finora
- HLTA02H3 - Lecture 4Documento14 pagineHLTA02H3 - Lecture 4Laura RudmikNessuna valutazione finora
- Den PubDocumento31 pagineDen PubEsperlyn SorianoNessuna valutazione finora
- Psychosocial Dynamic ManojDocumento37 paginePsychosocial Dynamic ManojVivion JacobNessuna valutazione finora
- Global Pattern of DiseaseDocumento40 pagineGlobal Pattern of DiseaseAlifa Nasyahta RosianaNessuna valutazione finora
- PPP Revision: Determinants of HealthDocumento11 paginePPP Revision: Determinants of HealthAishaNessuna valutazione finora
- Epidemiologi: Titiek Hidayati Dr. M. Kes. Dept. Epidemiologi, Kedokteran Masyarakat Dan KeluargaDocumento73 pagineEpidemiologi: Titiek Hidayati Dr. M. Kes. Dept. Epidemiologi, Kedokteran Masyarakat Dan KeluargaTrikz Vold LicickNessuna valutazione finora
- PRC Ple Review 021318Documento301 paginePRC Ple Review 021318Maria Cecilia Luz Romero67% (6)
- Epid SeluruhnyaDocumento43 pagineEpid SeluruhnyaAinun MahtobNessuna valutazione finora
- The Essential Role of The Nurse in Improving Health OutcomesDocumento38 pagineThe Essential Role of The Nurse in Improving Health OutcomesYAMINIPRIYANNessuna valutazione finora
- Dis Caus 2013 DesignDocumento157 pagineDis Caus 2013 DesignSarina AsuncionNessuna valutazione finora
- 2020 Disease Detectives 071619Documento71 pagine2020 Disease Detectives 071619Sharynn Kew MooreNessuna valutazione finora
- BIOS1054 What Is Health 26102023Documento27 pagineBIOS1054 What Is Health 261020230R4NG3Nessuna valutazione finora
- Wrap Up: Semester 3 - 2017Documento35 pagineWrap Up: Semester 3 - 2017AnggaNessuna valutazione finora
- Week 5 CHNDocumento147 pagineWeek 5 CHNJelliNessuna valutazione finora
- Epidemiology Week7 chn2 Aidavg Sept272020Documento131 pagineEpidemiology Week7 chn2 Aidavg Sept272020folkloriantaroNessuna valutazione finora
- DX KomunitasDocumento34 pagineDX KomunitasArin Nanda Sekar PalupiNessuna valutazione finora
- Disease Prevention and Control ### 2Documento33 pagineDisease Prevention and Control ### 2حنين إبراهيمNessuna valutazione finora
- Costy Pandjaitan, SKM.,MARSDocumento49 pagineCosty Pandjaitan, SKM.,MARSAmna RestiNessuna valutazione finora
- Evolution's Clinical Guidebook: Translating Ancient Genes into Precision MedicineDa EverandEvolution's Clinical Guidebook: Translating Ancient Genes into Precision MedicineNessuna valutazione finora
- Acute Chest PainDocumento45 pagineAcute Chest PainJonathan DavidNessuna valutazione finora
- Pad 120821Documento54 paginePad 120821Jonathan DavidNessuna valutazione finora
- 1st Month AssessmentDocumento43 pagine1st Month AssessmentJonathan DavidNessuna valutazione finora
- Treasure Hunt CluesDocumento4 pagineTreasure Hunt CluesJonathan DavidNessuna valutazione finora
- Claims and ArgumentsDocumento28 pagineClaims and ArgumentsJonathan DavidNessuna valutazione finora
- ChunkingDocumento15 pagineChunkingJonathan DavidNessuna valutazione finora
- Kirchoff's LawDocumento3 pagineKirchoff's LawJonathan DavidNessuna valutazione finora
- Dr. Ayu Swandewi A, MPHDocumento30 pagineDr. Ayu Swandewi A, MPHJonathan DavidNessuna valutazione finora
- Schaum S Outline of College Physics 9th Ed Bueche Hecht 0070089418Documento4 pagineSchaum S Outline of College Physics 9th Ed Bueche Hecht 0070089418Jonathan DavidNessuna valutazione finora
- Data Presentation and Data Description EngDocumento38 pagineData Presentation and Data Description EngJonathan DavidNessuna valutazione finora
- S A Pharmacy ListDocumento3 pagineS A Pharmacy Listjloco1904Nessuna valutazione finora
- Cervical CancerDocumento30 pagineCervical Cancerhuhknee100% (1)
- Block 1 PDFDocumento388 pagineBlock 1 PDFShubham ShuklaNessuna valutazione finora
- Jazper Final CaseDocumento7 pagineJazper Final CaseWynJoy NebresNessuna valutazione finora
- Dengue 20230427Documento11 pagineDengue 20230427Ariana hazelNessuna valutazione finora
- KDocumento10 pagineKVikas SinghNessuna valutazione finora
- Dengue Control ProgramDocumento2 pagineDengue Control ProgramJeanne Mari CostalesNessuna valutazione finora
- Partographic Analysis of Labour by Modified Who Partograph in Primigravidae: A Prospective Observational StudyDocumento4 paginePartographic Analysis of Labour by Modified Who Partograph in Primigravidae: A Prospective Observational StudyDarmawanNessuna valutazione finora
- Maternal and Child Nursing - Postpartum CareDocumento54 pagineMaternal and Child Nursing - Postpartum Carechuppepay33% (3)
- Group Task-Topic SentenceDocumento2 pagineGroup Task-Topic SentenceajengdwiprasantiNessuna valutazione finora
- Maternity and Child Health Nursing Gynaecology Report (Out Patient)Documento9 pagineMaternity and Child Health Nursing Gynaecology Report (Out Patient)Faizah AlshehriNessuna valutazione finora
- FC - CDDocumento27 pagineFC - CDCake ManNessuna valutazione finora
- Reviewing School Uniform Through A Public Health Lens: Evidence About The Impacts of School Uniform On Education and HealthDocumento17 pagineReviewing School Uniform Through A Public Health Lens: Evidence About The Impacts of School Uniform On Education and HealthJazpel NucupNessuna valutazione finora
- Expanded SurveillanceDocumento18 pagineExpanded SurveillanceSHILOTANessuna valutazione finora
- Chapter 18 Communicable Diseases PDFDocumento30 pagineChapter 18 Communicable Diseases PDFcelloguy8Nessuna valutazione finora
- General Objecti-Wps OfficeDocumento3 pagineGeneral Objecti-Wps OfficeSumit YadavNessuna valutazione finora
- Cardiovascular Disorder Case Study - EditedDocumento4 pagineCardiovascular Disorder Case Study - EditedTimohNessuna valutazione finora
- V2 VC 25.01.2020-1Documento134 pagineV2 VC 25.01.2020-1NandhiniNessuna valutazione finora
- E.-coli-Q & A From LehiDocumento3 pagineE.-coli-Q & A From LehiLarryDCurtisNessuna valutazione finora
- Gondiya MTPDocumento1 paginaGondiya MTPAbhishek Motiram JagtapNessuna valutazione finora
- Uganda National Medicines Policy, 2015Documento52 pagineUganda National Medicines Policy, 2015African Centre for Media ExcellenceNessuna valutazione finora
- Typhoid Fever at A GlanceDocumento2 pagineTyphoid Fever at A GlanceLIZNessuna valutazione finora
- Focus On Nursing Pharmacology Karch 5th Edition Test BankDocumento16 pagineFocus On Nursing Pharmacology Karch 5th Edition Test BankPeggie Edwards100% (31)
- Missed Abortion CaseDocumento6 pagineMissed Abortion Casekiyumi 132Nessuna valutazione finora
- Ethiopia Health Sector Transformation ProcessDocumento184 pagineEthiopia Health Sector Transformation ProcessAbebe TilahunNessuna valutazione finora
- Executive Summary Isolation Precaution ToolkitDocumento12 pagineExecutive Summary Isolation Precaution Toolkitwaqas_xsNessuna valutazione finora
- Human Health Risk AssessmentDocumento4 pagineHuman Health Risk AssessmentfakharNessuna valutazione finora
- True or FalseDocumento12 pagineTrue or Falsesweetescape1Nessuna valutazione finora
- JJ Fact Sheet RecipientsDocumento7 pagineJJ Fact Sheet RecipientsAlyssa RobertsNessuna valutazione finora
- Birth Control PillsDocumento2 pagineBirth Control PillsCharlizze ZafeNessuna valutazione finora