Potrebbero piacerti anche
- Psychotropic MedicationsDocumento37 paginePsychotropic MedicationsJoanne Bernadette AguilarNessuna valutazione finora
- Psychotropic Drugs.Documento15 paginePsychotropic Drugs.Xiaoqing SongNessuna valutazione finora
- 01 - Pharmacotherapy Pearls For Emergency Neurological Life Support PDFDocumento26 pagine01 - Pharmacotherapy Pearls For Emergency Neurological Life Support PDFawinsyNessuna valutazione finora
- ATI Flash Cards 05, Medications Affecting The Nervous SystemDocumento110 pagineATI Flash Cards 05, Medications Affecting The Nervous SystemGiovanni MictilNessuna valutazione finora
- Laporan Igd 2018Documento216 pagineLaporan Igd 2018Rahma watiNessuna valutazione finora
- Precedex Dosing GuidelinesDocumento15 paginePrecedex Dosing GuidelinesemonhalimNessuna valutazione finora
- DiazepamDocumento1 paginaDiazepamIvanne Hisoler71% (7)
- Mechanism of Action For Each Class of AntiDocumento146 pagineMechanism of Action For Each Class of AntiReynaldo RiveraNessuna valutazione finora
- Ecart MedicationsDocumento39 pagineEcart Medicationsanon_140774008Nessuna valutazione finora
- Beating the Benzo Blues: Getting off BenzodiazapinesDa EverandBeating the Benzo Blues: Getting off BenzodiazapinesValutazione: 5 su 5 stelle5/5 (1)
- Intravenous Anesthetic Agents-1Documento65 pagineIntravenous Anesthetic Agents-1Fauzan FajarNessuna valutazione finora
- AEMT Medication AdministrationDocumento24 pagineAEMT Medication AdministrationEmily KeenNessuna valutazione finora
- AdenosineDocumento2 pagineAdenosinegovind_soni_150% (1)
- AmobarbitalDocumento2 pagineAmobarbitalidullrufaidahNessuna valutazione finora
- KetamineDocumento2 pagineKetamineyanti anggrenie100% (1)
- Drug StudyDocumento4 pagineDrug Studyjazmine_caritos100% (2)
- 4 SeizuresDocumento11 pagine4 SeizuresApple MaeNessuna valutazione finora
- Reporting On IV AnestheticsDocumento88 pagineReporting On IV AnestheticsPaul Rizel LedesmaNessuna valutazione finora
- LorazepamDocumento3 pagineLorazepamgovind_soni_15Nessuna valutazione finora
- MastectomyDocumento53 pagineMastectomyAngelica RelanaNessuna valutazione finora
- AnxiolyticsDocumento56 pagineAnxiolyticsjabari.baraNessuna valutazione finora
- Critical Care Drugs 1Documento21 pagineCritical Care Drugs 1Asri ErnadiNessuna valutazione finora
- Chlorpromazine Drug StudyDocumento10 pagineChlorpromazine Drug Studyshadow gonzalezNessuna valutazione finora
- Critical Care Nursing Diagnosis and Management UrdenDocumento8 pagineCritical Care Nursing Diagnosis and Management UrdenMonet0% (1)
- Anesthetic AgentsDocumento7 pagineAnesthetic AgentsJan DacioNessuna valutazione finora
- PropofolDocumento3 paginePropofolamelwd100% (1)
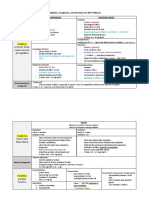
- Sedation, Analgesics, and Paralysis For MV Patients: Sedatives Promote Sleep, Reduce Anxiety and AgitationDocumento3 pagineSedation, Analgesics, and Paralysis For MV Patients: Sedatives Promote Sleep, Reduce Anxiety and Agitationفاطِمه سيد ابراهيمNessuna valutazione finora
- Drug StudyDocumento17 pagineDrug StudyJam CorrosNessuna valutazione finora
- Procedural SedationDocumento9 pagineProcedural SedationZayar SweNessuna valutazione finora
- Adult: IV/IM 5-10 MG, Drowsiness, Fatigue, Ataxia,: Injectable Form: ShockDocumento1 paginaAdult: IV/IM 5-10 MG, Drowsiness, Fatigue, Ataxia,: Injectable Form: ShockinfectionmanNessuna valutazione finora
- Anesthesia PharmacologyDocumento12 pagineAnesthesia PharmacologyMagy SnowNessuna valutazione finora
- Procedural Sedation Meds: Ketamine Management of ComplicationsDocumento2 pagineProcedural Sedation Meds: Ketamine Management of ComplicationsLile ArrisanNessuna valutazione finora
- Anesthesia Drugs Cheat SheetDocumento10 pagineAnesthesia Drugs Cheat Sheetapolan2Nessuna valutazione finora
- Dosage & RouteDocumento1 paginaDosage & RoutepiasolNessuna valutazione finora
- Anxiolytic DrugDocumento3 pagineAnxiolytic DrugAnna Mendiola-BasbasNessuna valutazione finora
- Kineme Case StudyDocumento8 pagineKineme Case Studyislafab25Nessuna valutazione finora
- Drug StudyDocumento12 pagineDrug Studyjoaqiun100% (1)
- DroperidolDocumento1 paginaDroperidolIvanne HisolerNessuna valutazione finora
- Week 7 Course TaskDocumento13 pagineWeek 7 Course TaskRachelle CambaNessuna valutazione finora
- Drug Study: Epinephrine: RecommendedDocumento5 pagineDrug Study: Epinephrine: RecommendedShara Lailanie A. AzisNessuna valutazione finora
- 2018-2019 Cns DepressantsDocumento5 pagine2018-2019 Cns DepressantsMary AgorillaNessuna valutazione finora
- DiazepamDocumento7 pagineDiazepamنمر نصارNessuna valutazione finora
- Pharmacology in NursingDocumento1 paginaPharmacology in NursingJessa Mae Barquilla100% (1)
- ClonazepamDocumento3 pagineClonazepamShane Shaira G PantaleonNessuna valutazione finora
- Lui Sh-Colored Lips and Finger Nails Blur Red VisionDocumento1 paginaLui Sh-Colored Lips and Finger Nails Blur Red VisionMagdayao Romamea100% (1)
- Metocloprramide HydrochlorideDocumento2 pagineMetocloprramide HydrochlorideBeatrizz P GellaNessuna valutazione finora
- Drugs For Anxiety and InsomniaDocumento10 pagineDrugs For Anxiety and InsomniaApple MaeNessuna valutazione finora
- CNS Depressants - Anxiolytics & Sedative HypnoticsDocumento4 pagineCNS Depressants - Anxiolytics & Sedative HypnoticsJustin HulinNessuna valutazione finora
- DiazepamDocumento2 pagineDiazepamBIRIN, JEHAN KAYLE T.Nessuna valutazione finora
- Benzodiazepines + Local AnesthesiaDocumento5 pagineBenzodiazepines + Local AnesthesiaALNAKINessuna valutazione finora
- Drug StudyDocumento6 pagineDrug StudyLovelyNessuna valutazione finora
- Shared AirwayDocumento5 pagineShared AirwayVictoria MedfordNessuna valutazione finora
- Psychopharmacological AgentsDocumento44 paginePsychopharmacological Agentsbazet49Nessuna valutazione finora
- AnxiolyticsDocumento8 pagineAnxiolyticsAlfie16Nessuna valutazione finora
- Adiel Joy P. Calsa Drug TabulationDocumento6 pagineAdiel Joy P. Calsa Drug TabulationAdiel CalsaNessuna valutazione finora
- AssignmentDocumento14 pagineAssignmentKimberly Claire DegalaNessuna valutazione finora
- EpinephrineDocumento4 pagineEpinephrinegovind_soni_15Nessuna valutazione finora
- Any Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently ReceivingDocumento1 paginaAny Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently Receivinggeorgeloto12Nessuna valutazione finora
- Injections: 2.5mg/ml in CNS: Drowsiness,: DroperidolDocumento3 pagineInjections: 2.5mg/ml in CNS: Drowsiness,: DroperidolthesarayoNessuna valutazione finora
- AirwaydrugsDocumento5 pagineAirwaydrugshevere6273Nessuna valutazione finora
- Mental HealthDocumento6 pagineMental HealtholadapoNessuna valutazione finora
- Conscious Sedation: Prof - Med. Nabil H. Mohyeddin Intensive Care &anesthesiologyDocumento84 pagineConscious Sedation: Prof - Med. Nabil H. Mohyeddin Intensive Care &anesthesiologyKhaled GharaibehNessuna valutazione finora
- DRUG STUDY - AnticonvulsantsDocumento1 paginaDRUG STUDY - AnticonvulsantsZam PamateNessuna valutazione finora
- AnxietyDocumento6 pagineAnxietyMasa MasaNessuna valutazione finora
- Mid FastDocumento30 pagineMid FastsujitmandotNessuna valutazione finora
- Week 5 - Course TaskDocumento7 pagineWeek 5 - Course TaskCher Allain BellosilloNessuna valutazione finora
- Er-Drug StudyDocumento41 pagineEr-Drug Studyrc_lacampuinganyahooNessuna valutazione finora
- Drug Study A.Documento14 pagineDrug Study A.Yshy LingadNessuna valutazione finora
- Any Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently ReceivingDocumento1 paginaAny Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently Receivinggeorgeloto12Nessuna valutazione finora
- Medical Emergencies in The Dental Surgery20.11.08Documento21 pagineMedical Emergencies in The Dental Surgery20.11.08Yusuf KozniewskiNessuna valutazione finora
- Status EpileptikusDocumento5 pagineStatus EpileptikusspiritNessuna valutazione finora
- Controlled Substances: Standard Operating Procedure #401Documento8 pagineControlled Substances: Standard Operating Procedure #401bishopNessuna valutazione finora
- Emergency Drugs and Calculations: Thavamani KandasamyDocumento24 pagineEmergency Drugs and Calculations: Thavamani Kandasamypaulyn ramos100% (1)
- High Alert DrugsDocumento17 pagineHigh Alert DrugsAndrean Mukti BeladexsaNessuna valutazione finora
- Guideline For Endoscopy in Pregnant and Lactating WomenDocumento6 pagineGuideline For Endoscopy in Pregnant and Lactating WomenRommel YánacNessuna valutazione finora
- Intravenous Infusion of Lidocaine Reduces PropofolDocumento6 pagineIntravenous Infusion of Lidocaine Reduces PropofolAnonymous lSWQIQNessuna valutazione finora
- General Anesthesia 1 PDFDocumento49 pagineGeneral Anesthesia 1 PDFYokita JanarthananNessuna valutazione finora
- Anestesia de EquinosDocumento9 pagineAnestesia de EquinosKiimBerly RcNessuna valutazione finora
- A Gastroenterologist's Guide To Gut Health-Novick-2017Documento257 pagineA Gastroenterologist's Guide To Gut Health-Novick-2017Engin UçarNessuna valutazione finora
- VersedDocumento2 pagineVersedNinoska Garcia-Ortiz100% (3)
- Dexmedetomidina en Anestesia PediatricaDocumento11 pagineDexmedetomidina en Anestesia PediatricaRodolfo MarinNessuna valutazione finora
- Multiple Choice Questions: Childhood Obesity and The AnaesthetistDocumento5 pagineMultiple Choice Questions: Childhood Obesity and The AnaesthetistTanishka GargNessuna valutazione finora
- 04 P006 12786Documento8 pagine04 P006 12786bijoy82Nessuna valutazione finora
- CMR SedationDocumento2 pagineCMR SedationYong Wai100% (1)
- Status Epilepticus: by Aaron M. Cook, Pharm.D., BCPS, BCCCPDocumento20 pagineStatus Epilepticus: by Aaron M. Cook, Pharm.D., BCPS, BCCCPpuaanNessuna valutazione finora
- Full Controlled Check ListDocumento2 pagineFull Controlled Check ListvyshnosudhaNessuna valutazione finora
- Proforma For Registration of Subjects For Dissertation: Appendix-IcDocumento32 pagineProforma For Registration of Subjects For Dissertation: Appendix-IcRahul KambleNessuna valutazione finora
- Paediatric Sedation: Michael R. J. Sury FRCADocumento5 paginePaediatric Sedation: Michael R. J. Sury FRCASantosa TandiNessuna valutazione finora
- Factsheet 9 On Palliative Care Terminal RestlessnessDocumento2 pagineFactsheet 9 On Palliative Care Terminal RestlessnessvabcunhaNessuna valutazione finora