Potrebbero piacerti anche
- Diabetic Recipes for One and TwoDa EverandDiabetic Recipes for One and TwoValutazione: 3 su 5 stelle3/5 (1)
- Diabetes: Reverse Your Diabetes With a Clear and Concise Step by Step GuideDa EverandDiabetes: Reverse Your Diabetes With a Clear and Concise Step by Step GuideValutazione: 3 su 5 stelle3/5 (1)
- Pemeriksaan Visus Bayi & AnakDocumento26 paginePemeriksaan Visus Bayi & AnakMelinda Balqis Annur ZahwaNessuna valutazione finora
- Early Detection and Standardized Diabetes ManagementDocumento26 pagineEarly Detection and Standardized Diabetes ManagementKoas NeurologiNessuna valutazione finora
- Seminar DM Bpjs Juni 2014Documento28 pagineSeminar DM Bpjs Juni 2014Ari AsriniNessuna valutazione finora
- Himawan - BPJSDocumento26 pagineHimawan - BPJSAndi Upik FathurNessuna valutazione finora
- Jack Leahy Insulin TherapyDocumento44 pagineJack Leahy Insulin TherapyFrancisNessuna valutazione finora
- Glucose Tolerance TestDocumento27 pagineGlucose Tolerance Testsiya sharmaNessuna valutazione finora
- Drugs Used in Treatment of Diabetes MellitusDocumento38 pagineDrugs Used in Treatment of Diabetes MellitusMohammad Hazamyn Hazrul HamzahNessuna valutazione finora
- Lecture 2 Diabetes Mellitus TherapyDocumento155 pagineLecture 2 Diabetes Mellitus Therapyaleen qawareet100% (1)
- Management of Type 2 Diabetes:: DR - Bratasena.Mkedpd - SPPDDocumento51 pagineManagement of Type 2 Diabetes:: DR - Bratasena.Mkedpd - SPPDAnnisa SyafeiNessuna valutazione finora
- Insulin GNTDocumento41 pagineInsulin GNTV Narayan Rao TummalaNessuna valutazione finora
- Penanganan DMDocumento28 paginePenanganan DMbe a doctor for you Medical studentNessuna valutazione finora
- Diabetes Mellitus: Anne Dawnay Biochemical MedicineDocumento26 pagineDiabetes Mellitus: Anne Dawnay Biochemical MedicineJoni HermawanNessuna valutazione finora
- Referat DM Mooi FixDocumento54 pagineReferat DM Mooi FixKhansadhia Hasmaradana Mooiindie DjojonegoroNessuna valutazione finora
- Diabetes Mellitus: Dr. Stanley Binagi Mmed Internal MedicineDocumento60 pagineDiabetes Mellitus: Dr. Stanley Binagi Mmed Internal MedicineTeddy MauriceNessuna valutazione finora
- Diabetes Mellitus2Documento26 pagineDiabetes Mellitus2Rhei Danganan-MercadoNessuna valutazione finora
- DIABETES MELLITUS FinalDocumento83 pagineDIABETES MELLITUS FinalYuvi Yuvaraj100% (1)
- Materi Diabetes Mellitus - WAHYUDocumento29 pagineMateri Diabetes Mellitus - WAHYUAli Sibra MulluziNessuna valutazione finora
- DiabetesDocumento99 pagineDiabetes489226fahimNessuna valutazione finora
- Treatment of Diabetic MellitusDocumento40 pagineTreatment of Diabetic MellitusAnis Eka SukmadadariNessuna valutazione finora
- Diabetes UGDocumento34 pagineDiabetes UGRecovery MailNessuna valutazione finora
- What Is Diabetes (PSEm) 02 - 2Documento41 pagineWhat Is Diabetes (PSEm) 02 - 2tridewantiwNessuna valutazione finora
- Diabetes Management With Basal InsulinDocumento35 pagineDiabetes Management With Basal InsulinSultan MubashirNessuna valutazione finora
- Wira Gotera, DR, DR, SPPD, Kemd, Finasim Kosultan Senior, Divisi Metabolik Dan Endokrin FK Udayana-RSUP Sanglah DenpasarDocumento53 pagineWira Gotera, DR, DR, SPPD, Kemd, Finasim Kosultan Senior, Divisi Metabolik Dan Endokrin FK Udayana-RSUP Sanglah DenpasarRetno handayani PDNessuna valutazione finora
- The Role of Rapid Insulin Analogue in Diabetes Management Focused On Glulisine Clinical EvidenceDocumento34 pagineThe Role of Rapid Insulin Analogue in Diabetes Management Focused On Glulisine Clinical EvidenceAnonymous iIwZjFpbVNessuna valutazione finora
- Diabetes - Mellitus - 1 - Y2 - 280915Documento24 pagineDiabetes - Mellitus - 1 - Y2 - 280915azizan hannyNessuna valutazione finora
- Path122 Diabetes MellitusDocumento12 paginePath122 Diabetes MellitusGwendolaine PicaNessuna valutazione finora
- Diabetes - Oral KnowledgeDocumento19 pagineDiabetes - Oral KnowledgeKSeegurNessuna valutazione finora
- DM Presentation NewDocumento44 pagineDM Presentation NewKipz JonsNessuna valutazione finora
- PP Lantus & Apidra ID Dokter. Update Insulin in RamadhanDocumento57 paginePP Lantus & Apidra ID Dokter. Update Insulin in RamadhanAhmad Husain 'Ucenk' PalliNessuna valutazione finora
- Beyond Insulin Resistance: Islet Cells As Key Drivers in Type 2 DMDocumento16 pagineBeyond Insulin Resistance: Islet Cells As Key Drivers in Type 2 DMBeta Cells in DiabetesNessuna valutazione finora
- Diabetes Mellitus: Rahayu Setyowati, Skp.,MkepDocumento47 pagineDiabetes Mellitus: Rahayu Setyowati, Skp.,MkepNurul asriNessuna valutazione finora
- Diabetes Mellitus: Dr. Sajid Abbas JaffriDocumento37 pagineDiabetes Mellitus: Dr. Sajid Abbas JaffriMaham ZarrinNessuna valutazione finora
- Diabetes Mellitus: Shahrul RahmanDocumento80 pagineDiabetes Mellitus: Shahrul RahmanMunawwar AweNessuna valutazione finora
- 1.PERKENI 22-23 JUNI2019-Practical Aspect of Using InsulinDocumento21 pagine1.PERKENI 22-23 JUNI2019-Practical Aspect of Using InsulinFloreanHartungiLotisnaNessuna valutazione finora
- Diabetes Mellitus: Dr. Beny Ghufron, SP - PD. SMF Penyakit Dalam Rsud DR Haryoto LumajangDocumento70 pagineDiabetes Mellitus: Dr. Beny Ghufron, SP - PD. SMF Penyakit Dalam Rsud DR Haryoto LumajangDendian Berlia JelitaNessuna valutazione finora
- Kegawatdaruratan Diabetes Melitus: Terapi Insulin IntravenaDocumento27 pagineKegawatdaruratan Diabetes Melitus: Terapi Insulin IntravenaSesilia Sri Yanti GaddyNessuna valutazione finora
- Seminar DM BPJS Gresik 07092017 (Dr. Hermina)Documento37 pagineSeminar DM BPJS Gresik 07092017 (Dr. Hermina)Ali Sibra MulluziNessuna valutazione finora
- Dsa 698Documento12 pagineDsa 698Mwanja MosesNessuna valutazione finora
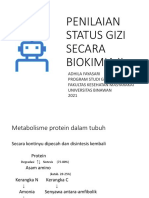
- 12 PSG-Pemeriksaan Biokimia-II Karbohidrat Lemak ProteinDocumento48 pagine12 PSG-Pemeriksaan Biokimia-II Karbohidrat Lemak ProteinTyas PutriNessuna valutazione finora
- The Role of Insulin Premix 50 in DM Type 2 Management DR OnggoDocumento31 pagineThe Role of Insulin Premix 50 in DM Type 2 Management DR Onggoong251183Nessuna valutazione finora
- Adobe Scan 4 Nov 2023Documento10 pagineAdobe Scan 4 Nov 2023riddhimithastalinNessuna valutazione finora
- Curs Diabet 1-3Documento202 pagineCurs Diabet 1-3serj_inaNessuna valutazione finora
- Adult Onset Diabetes Mellitus Management Options: DR Muhammad Israr Ul HaqDocumento88 pagineAdult Onset Diabetes Mellitus Management Options: DR Muhammad Israr Ul HaqMuhammad Israr Ul HaqNessuna valutazione finora
- Tatalaksana Diabetes Pada Pelayanan PrimerDocumento49 pagineTatalaksana Diabetes Pada Pelayanan PrimerEvri LiaNessuna valutazione finora
- Patofisiologi DMDocumento26 paginePatofisiologi DMMunawwar AweNessuna valutazione finora
- Hypertension & Diabetis MellitusDocumento51 pagineHypertension & Diabetis MellitusSuma_Ramesan_5373100% (1)
- 4.release How To Intensify Basal Insulin With Premix and Basal Bolus ApproachDocumento42 pagine4.release How To Intensify Basal Insulin With Premix and Basal Bolus ApproachaprinaaaNessuna valutazione finora
- Welcome To The PresentationDocumento32 pagineWelcome To The PresentationIshaan Arfatur Rahman0% (1)
- Diabetes Mellitus Final SibiDocumento62 pagineDiabetes Mellitus Final SibiSibi JohnNessuna valutazione finora
- Cinical Inertia - Final Release PDFDocumento43 pagineCinical Inertia - Final Release PDFrent3010Nessuna valutazione finora
- Nutrisi Pada DMDocumento48 pagineNutrisi Pada DMalwiNessuna valutazione finora
- Endocrine Emergencies: Dr. Diyah Saraswati, SPPDDocumento21 pagineEndocrine Emergencies: Dr. Diyah Saraswati, SPPDAhmad AgielNessuna valutazione finora
- Penggunaan Insulin Pada Diabetes Tipe 2Documento47 paginePenggunaan Insulin Pada Diabetes Tipe 2pebbyfebrianNessuna valutazione finora
- Random Blood Sugar Test: - Two Columns - One ColumnDocumento7 pagineRandom Blood Sugar Test: - Two Columns - One ColumnMattNessuna valutazione finora
- CukrzycaDocumento52 pagineCukrzycatyhbbhhNessuna valutazione finora
- 2023 Diabetes MellitusDocumento138 pagine2023 Diabetes Mellitusmerga wekwayaNessuna valutazione finora
- Diabetes Mellitus LectureDocumento68 pagineDiabetes Mellitus LectureDikyAksiramNessuna valutazione finora
- Presented by DR Ashish Sharma Guided by DR Meena PatelDocumento74 paginePresented by DR Ashish Sharma Guided by DR Meena PatelAndrew Surya Putra SccNessuna valutazione finora
- LP U1209300 Inoa 2013 Inoa Color ChartDocumento4 pagineLP U1209300 Inoa 2013 Inoa Color ChartbinreNessuna valutazione finora
- Nursing TheoryDocumento13 pagineNursing TheoryYana VictyNessuna valutazione finora
- 365 Land Transport SafetyDocumento24 pagine365 Land Transport Safetyleo limpiasNessuna valutazione finora
- Formulasi Fast Desintegrating Tablet (FDT) Sari Buah Jambu Biji Merah Dengan Perbedaan Konsentrasi Ac-DisolDocumento8 pagineFormulasi Fast Desintegrating Tablet (FDT) Sari Buah Jambu Biji Merah Dengan Perbedaan Konsentrasi Ac-Disolfauzul husnaNessuna valutazione finora
- 51 - Methemoglobin ProducersDocumento20 pagine51 - Methemoglobin ProducersCabinet VeterinarNessuna valutazione finora
- Roche Chemstrip 2 Insert Instruction SheetDocumento2 pagineRoche Chemstrip 2 Insert Instruction SheetEveyNessuna valutazione finora
- Students' Nutrition - School Canteen Affecting Their Food ChoiceDocumento19 pagineStudents' Nutrition - School Canteen Affecting Their Food ChoicesamantaNessuna valutazione finora
- (Becker, 2009) Satulogenesis 30 Years LaterDocumento8 pagine(Becker, 2009) Satulogenesis 30 Years LaterZooTEKNessuna valutazione finora
- Nurses Role in Drug Therapy: BY Puan Haslinda Binti Dan NURSING BLOCK 2008/2009Documento40 pagineNurses Role in Drug Therapy: BY Puan Haslinda Binti Dan NURSING BLOCK 2008/2009Rhomizal MazaliNessuna valutazione finora
- Rewire Your BrainDocumento0 pagineRewire Your BrainJohn Bates100% (1)
- Pathophysiology of GastroenteritisDocumento2 paginePathophysiology of GastroenteritisJun MingNessuna valutazione finora
- Cambios Tranvversales, Verticales Anclaje Oseo VS DentosoportadoDocumento12 pagineCambios Tranvversales, Verticales Anclaje Oseo VS DentosoportadoLAURA MARCELA BARRENECHE CALLENessuna valutazione finora
- IVT Network - Process Validation - 2014-04-28Documento1 paginaIVT Network - Process Validation - 2014-04-28Mina Maher MikhailNessuna valutazione finora
- 30 BÀI LUẬN MẪU DÀNH CHO HS CẤP 2Documento7 pagine30 BÀI LUẬN MẪU DÀNH CHO HS CẤP 2Đào Thị HảiNessuna valutazione finora
- Wintrobe Anemia On Chronic DiseaseDocumento31 pagineWintrobe Anemia On Chronic DiseaseDistro ThedocsNessuna valutazione finora
- Dr-Nursing Care PlanDocumento2 pagineDr-Nursing Care PlanKhrisha Anne Davillo100% (1)
- Dukungan Sosial Dan Post-Traumatic Stress DisorderDocumento7 pagineDukungan Sosial Dan Post-Traumatic Stress DisordercholiidNessuna valutazione finora
- Chapter 3 The Molecules of CellsDocumento5 pagineChapter 3 The Molecules of Cellsmzunl25476Nessuna valutazione finora
- Mark Lyons 2010Documento11 pagineMark Lyons 2010Drosler MedqsNessuna valutazione finora
- 3.1.1.3 CONTOH Pedoman Manual Mutu OKKKKDocumento39 pagine3.1.1.3 CONTOH Pedoman Manual Mutu OKKKKsapnah SKM100% (1)
- Hand Assessment - 3rd YrDocumento54 pagineHand Assessment - 3rd YrSURBHI AGRAWALNessuna valutazione finora
- Persuasive Essay On Weed LegalizationDocumento6 paginePersuasive Essay On Weed LegalizationAlyssa HilliardNessuna valutazione finora
- Intermediate 3 - Workbook - Updated 2017Documento107 pagineIntermediate 3 - Workbook - Updated 2017Techbort TechnortNessuna valutazione finora
- The Statistical Abstract of The United States 2009Documento996 pagineThe Statistical Abstract of The United States 2009Aaron MonkNessuna valutazione finora
- PolicyDocumento5 paginePolicySriharsha ReddyNessuna valutazione finora
- Otda Foil Request 2Documento4 pagineOtda Foil Request 2sammyschwartz08Nessuna valutazione finora
- PacmakerDocumento37 paginePacmakerSalman HabeebNessuna valutazione finora
- 2020-04-08 A New World Through My Window - Olga TokarczukDocumento4 pagine2020-04-08 A New World Through My Window - Olga TokarczukNatalia CimoNessuna valutazione finora
- Blood Groups PPT by TKR&SRDocumento24 pagineBlood Groups PPT by TKR&SRseshagiriNessuna valutazione finora
- Government of Kerala: Read 1 GO (RT) No. 396/2021/DMD Dated 03/05/2021Documento3 pagineGovernment of Kerala: Read 1 GO (RT) No. 396/2021/DMD Dated 03/05/2021hpindigo clubNessuna valutazione finora