Potrebbero piacerti anche
- Manual GPS Trimble Portugues CFX-750 / FM-750Documento246 pagineManual GPS Trimble Portugues CFX-750 / FM-750José Luis Mailkut Pires100% (5)
- Create PDF Book App in Android Studio - Download Free PDF Book Source Code PDFDocumento6 pagineCreate PDF Book App in Android Studio - Download Free PDF Book Source Code PDFshafiq09090% (1)
- Eva Braun Life With Hitler PDFDocumento2 pagineEva Braun Life With Hitler PDFPamela0% (1)
- Er 15-16 May 2017Documento96 pagineEr 15-16 May 2017ZakkyMaulanaRahmatNessuna valutazione finora
- ER 23-24 Juli 2016Documento55 pagineER 23-24 Juli 2016Theresia Alfionita SinulinggaNessuna valutazione finora
- Emergency Case TemplateDocumento46 pagineEmergency Case TemplateJacky JunaediNessuna valutazione finora
- Emergency Report: July 26 - July 27 2016Documento40 pagineEmergency Report: July 26 - July 27 2016Theresia Alfionita SinulinggaNessuna valutazione finora
- Emergency Room Morning Report: October 16th 2017Documento68 pagineEmergency Room Morning Report: October 16th 2017Rully SyahrizalNessuna valutazione finora
- Emergency Case Report 4 - 5 February 2019: TH THDocumento49 pagineEmergency Case Report 4 - 5 February 2019: TH THmonyet65Nessuna valutazione finora
- Emergency Case Report June 8 - 9 2019: TH THDocumento83 pagineEmergency Case Report June 8 - 9 2019: TH THEmma AssagafNessuna valutazione finora
- Slide MR 7 - 8 Agustus 2017Documento62 pagineSlide MR 7 - 8 Agustus 2017Heru WahyudiNessuna valutazione finora
- Wahidin Sudirohusodo Hospital, Tuesday 19th Oct 2021 (Period October 13th - October 17th 2021)Documento6 pagineWahidin Sudirohusodo Hospital, Tuesday 19th Oct 2021 (Period October 13th - October 17th 2021)MirahAvishaNessuna valutazione finora
- Rekapan Pembacaan Periode 05-25 Okt 2020Documento2 pagineRekapan Pembacaan Periode 05-25 Okt 2020joions gilberth oppiesNessuna valutazione finora
- Laporan Pagi Anestesi Operasi Cito: No Nama/Umur Diagnosis Tindakan Problem Prognosis ASA Jenis AnestesiDocumento1 paginaLaporan Pagi Anestesi Operasi Cito: No Nama/Umur Diagnosis Tindakan Problem Prognosis ASA Jenis AnestesiNovia Bintari NirmalasariNessuna valutazione finora
- Laporan Jaga Igd: Rsud Adhiyatma, MPH Coass Bedah UnimusDocumento27 pagineLaporan Jaga Igd: Rsud Adhiyatma, MPH Coass Bedah UnimusDony Hamonangan SiregarNessuna valutazione finora
- Wahidin Sudirohusodo Hospital / Nuraeni Period September 16 - September 19 2018Documento4 pagineWahidin Sudirohusodo Hospital / Nuraeni Period September 16 - September 19 2018dr_depeNessuna valutazione finora
- Resume DR RF 11102023Documento3 pagineResume DR RF 11102023bedahunand2023Nessuna valutazione finora
- Laporan Pagi Anestesi Operasi CitoDocumento2 pagineLaporan Pagi Anestesi Operasi CitoDita Garfield AssegafNessuna valutazione finora
- Laporan Pagi Anestesi Operasi ElektifDocumento2 pagineLaporan Pagi Anestesi Operasi ElektifAli AkbarNessuna valutazione finora
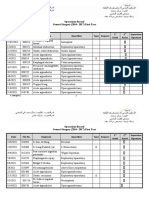
- Operations Record General Surgery (2016 - 2017) First YearDocumento2 pagineOperations Record General Surgery (2016 - 2017) First YeartameemNessuna valutazione finora
- Adobe Scan 15-Jul-2023Documento5 pagineAdobe Scan 15-Jul-2023PS CTKRNessuna valutazione finora
- Doctors On Duty: Saturday 06 TH July 2019Documento1 paginaDoctors On Duty: Saturday 06 TH July 2019Doctor's BettaNessuna valutazione finora
- No. Date of Admission Date of Discharge Patient Name (Age/LMP/MR) Detail of Patient (Treatment RecommendationDocumento3 pagineNo. Date of Admission Date of Discharge Patient Name (Age/LMP/MR) Detail of Patient (Treatment RecommendationAndi Tenri Ola Oddang IINessuna valutazione finora
- CARINA Final CasesDocumento5 pagineCARINA Final CasesmhynaNessuna valutazione finora
- No Name/Sex/Age Diagnose Icd X Treatment ICD IXDocumento2 pagineNo Name/Sex/Age Diagnose Icd X Treatment ICD IXDoctor's BettaNessuna valutazione finora
- Hosneara Begum - Aastha ConcentDocumento2 pagineHosneara Begum - Aastha ConcentAbul HasnatNessuna valutazione finora
- Wa0055.Documento2 pagineWa0055.subash boseNessuna valutazione finora
- OT List 25-10-2023Documento4 pagineOT List 25-10-2023ArhanNessuna valutazione finora
- CARINA Final CasesDocumento5 pagineCARINA Final CasesJeremiah M. MascariñasNessuna valutazione finora
- Surgeon Should Learn Not Just How To Operate But How To Create System of CareDocumento19 pagineSurgeon Should Learn Not Just How To Operate But How To Create System of Careamal.fathullahNessuna valutazione finora
- Orthopaedic Consultant Protocol (Otago) : ShoulderDocumento16 pagineOrthopaedic Consultant Protocol (Otago) : ShoulderAnonymous oROLLTxNessuna valutazione finora
- Surat IjinDocumento6 pagineSurat IjinNaeny FajriahNessuna valutazione finora
- MohammedDocumento75 pagineMohammedMuhammad SdiqNessuna valutazione finora
- R Schedule 2020 2021Documento1 paginaR Schedule 2020 2021Mohammed AhmedNessuna valutazione finora
- Adobe Scan 14 Apr 2024Documento1 paginaAdobe Scan 14 Apr 2024jaganpradhan847Nessuna valutazione finora
- Locandina ATTINGO 2014 - 15dic2203Documento2 pagineLocandina ATTINGO 2014 - 15dic2203Andrea PistochiniNessuna valutazione finora
- Dr. Rasul Dr. Orencia: Surgery ER Orthopedics Ward OR ENT OPD Ophthalmology ClerkDocumento12 pagineDr. Rasul Dr. Orencia: Surgery ER Orthopedics Ward OR ENT OPD Ophthalmology ClerkApmc SchwartzNessuna valutazione finora
- HIS DataDocumento2 pagineHIS DataAhmed AbuelezzNessuna valutazione finora
- Adobe Scan 18 Sep 2022Documento1 paginaAdobe Scan 18 Sep 2022sawtulhassanNessuna valutazione finora
- KARDEX (Admission)Documento1 paginaKARDEX (Admission)JA BerzabalNessuna valutazione finora
- Case 1Documento9 pagineCase 1Joselyn M. LachicaNessuna valutazione finora
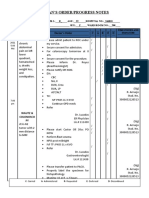
- Date Progress Notes Doctor's Order C AR E DDocumento4 pagineDate Progress Notes Doctor's Order C AR E DRenea Joy ArruejoNessuna valutazione finora
- Module 3 - Case 1Documento9 pagineModule 3 - Case 1Joselyn M. LachicaNessuna valutazione finora
- Module 2 - Case 1Documento9 pagineModule 2 - Case 1Joselyn M. LachicaNessuna valutazione finora
- Selama CC Berlangsung: No Cell Phone No CameraDocumento36 pagineSelama CC Berlangsung: No Cell Phone No CameraRadenSiwi Bagus HadhiningratNessuna valutazione finora
- Echa ReportmDocumento13 pagineEcha ReportmMohammad FarizNessuna valutazione finora
- Final CasesDocumento5 pagineFinal CasesKabang MoaNessuna valutazione finora
- Jadwal Operasi WorkshopDocumento3 pagineJadwal Operasi WorkshopM Halis HermawanNessuna valutazione finora
- KARDEX (Admission)Documento1 paginaKARDEX (Admission)JA BerzabalNessuna valutazione finora
- UTP Bishal AgrawalDocumento10 pagineUTP Bishal AgrawalbinarajpadhanNessuna valutazione finora
- Case Discussion in Oral SurgeryDocumento21 pagineCase Discussion in Oral SurgeryJosh Anthony Baker TañadaNessuna valutazione finora
- Wahidin Sudirohusodo Hospital / Gressella K. Mamangkey: Pre Operative DiagnosisDocumento6 pagineWahidin Sudirohusodo Hospital / Gressella K. Mamangkey: Pre Operative DiagnosisDwickyNessuna valutazione finora
- Jadwal Op. Sabtu, 21 Jan 2023Documento3 pagineJadwal Op. Sabtu, 21 Jan 2023M. Zuhdi HafizNessuna valutazione finora
- ROADMAP 2022: Published in Medical Buyer MagazineDocumento22 pagineROADMAP 2022: Published in Medical Buyer MagazinePushpanjali HospitalNessuna valutazione finora
- Grama TicaDocumento8 pagineGrama Ticaalejandra_baltaza_17Nessuna valutazione finora
- Purpose: To Compare Management Blepharoconjungtivitis in Steven Johnson SyndromeDocumento1 paginaPurpose: To Compare Management Blepharoconjungtivitis in Steven Johnson SyndromeHarmaini MemenNessuna valutazione finora
- Appeared at The Time of ArgumentsDocumento5 pagineAppeared at The Time of ArgumentsMoneylife FoundationNessuna valutazione finora
- Tplasty AishwaryaDocumento2 pagineTplasty Aishwaryaankitkawale111Nessuna valutazione finora
- History FormDocumento5 pagineHistory FormYazeed AsrawiNessuna valutazione finora
- Unit 6 Part 2 Table - Completed Fall 2023Documento2 pagineUnit 6 Part 2 Table - Completed Fall 2023Tanisha SheltonNessuna valutazione finora
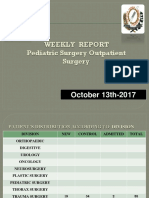
- Weekly Report Pediatric Surgery Outpatient Surgery: October 13th-2017Documento5 pagineWeekly Report Pediatric Surgery Outpatient Surgery: October 13th-2017Agung IgstNessuna valutazione finora
- GIN 2 IAN 28.01.2020 FixDocumento7 pagineGIN 2 IAN 28.01.2020 FixRyan IlhamNessuna valutazione finora
- Post-cholecystectomy Bile Duct InjuryDa EverandPost-cholecystectomy Bile Duct InjuryVinay K. KapoorNessuna valutazione finora
- Lpm2.1theoryDocumento85 pagineLpm2.1theoryvetprabu34Nessuna valutazione finora
- Drishti IasDocumento36 pagineDrishti Ias23010126269Nessuna valutazione finora
- Aporte Al IPSS Del Empleador Por TrabajadorDocumento4 pagineAporte Al IPSS Del Empleador Por Trabajadorvagonet21Nessuna valutazione finora
- CrossFit Wod Tracking JournalDocumento142 pagineCrossFit Wod Tracking JournalJavier Estelles Muñoz0% (1)
- Fruit LeathersDocumento4 pagineFruit LeathersAmmon FelixNessuna valutazione finora
- 6.4 Past Simple Affirmative: 0 Called HadDocumento1 pagina6.4 Past Simple Affirmative: 0 Called HadSashkaKoreckajaNessuna valutazione finora
- MLOG GX CMXA75 v4.05 322985e0 UM-EN PDFDocumento342 pagineMLOG GX CMXA75 v4.05 322985e0 UM-EN PDFGandalf cimarillonNessuna valutazione finora
- Aalborg Engineering Sg8 EngDocumento4 pagineAalborg Engineering Sg8 EngHenrique de OliveiraNessuna valutazione finora
- Joget Mini Case Studies TelecommunicationDocumento3 pagineJoget Mini Case Studies TelecommunicationavifirmanNessuna valutazione finora
- Factor Affecting Child Dental Behaviour PedoDocumento19 pagineFactor Affecting Child Dental Behaviour PedoFourthMolar.comNessuna valutazione finora
- Ed A 02.00 I 01Documento39 pagineEd A 02.00 I 01Enrique BlancoNessuna valutazione finora
- Kebutuhan Modal Kerja Pada Cv. Cipta Karya Mandiri Di SamarindaDocumento7 pagineKebutuhan Modal Kerja Pada Cv. Cipta Karya Mandiri Di SamarindaHerdi VhantNessuna valutazione finora
- Educational Institutions: Santos, Sofia Anne PDocumento11 pagineEducational Institutions: Santos, Sofia Anne PApril ManjaresNessuna valutazione finora
- Modelling The Relationship Between Hotel Perceived Value, CustomerDocumento11 pagineModelling The Relationship Between Hotel Perceived Value, Customerzoe_zoeNessuna valutazione finora
- Monthly Film Bulletin: 1T1IcqDocumento12 pagineMonthly Film Bulletin: 1T1IcqAlfred_HitzkopfNessuna valutazione finora
- Italian CuisineDocumento29 pagineItalian CuisinekresnayandraNessuna valutazione finora
- A Daily Miracle2Documento1 paginaA Daily Miracle2LizZelencichNessuna valutazione finora
- Online Gaming and Social BehaviorDocumento13 pagineOnline Gaming and Social BehaviorPave Llido100% (1)
- C Programming Bit Bank U-1, U-2Documento17 pagineC Programming Bit Bank U-1, U-2HariahNessuna valutazione finora
- Hellinger, Bert - GenoGraph 2.1 ManualDocumento16 pagineHellinger, Bert - GenoGraph 2.1 ManualGladys Achurra DíazNessuna valutazione finora
- APD6 Spec T20X en RevaDocumento10 pagineAPD6 Spec T20X en RevaKarla MartinsNessuna valutazione finora
- EARTH SCIENCE NotesDocumento8 pagineEARTH SCIENCE NotesAlthea Zen AyengNessuna valutazione finora
- 32 EM GreenTechDocumento45 pagine32 EM GreenTechMark Lester RealNessuna valutazione finora
- Fume Cup BrochureDocumento2 pagineFume Cup Brochuremfisol2000Nessuna valutazione finora
- Activity 1 Which Is WhichDocumento1 paginaActivity 1 Which Is WhichRhanna Lei SiaNessuna valutazione finora
- Making Electric Vehicles ProfitableDocumento18 pagineMaking Electric Vehicles ProfitablevjslkumarNessuna valutazione finora