Potrebbero piacerti anche
- Essential Treatment Guidelines for BronchopneumoniaDocumento67 pagineEssential Treatment Guidelines for BronchopneumoniaVerra AnindyaNessuna valutazione finora
- Bronkopneumonia Pada Pasien PediatrikDocumento5 pagineBronkopneumonia Pada Pasien PediatrikCecilia Evangelista NiluhNessuna valutazione finora
- CASE REPORT 4: PNEUMONIA DEXTRA SUSPECT COVID-19 + ACUTE GASTRITISDocumento17 pagineCASE REPORT 4: PNEUMONIA DEXTRA SUSPECT COVID-19 + ACUTE GASTRITISdianarahimmNessuna valutazione finora
- Bunga Rampai Infeksi Dengue AnakDocumento67 pagineBunga Rampai Infeksi Dengue AnakSatrio PrimaesoNessuna valutazione finora
- Pertanyaan Jurnal ReadingDocumento5 paginePertanyaan Jurnal ReadingMohammad AlmuhaiminNessuna valutazione finora
- Case Report on Pulmonary TuberculosisDocumento38 pagineCase Report on Pulmonary TuberculosisBunga Listia ParamitaNessuna valutazione finora
- Case Report BronkopneumoniaDocumento25 pagineCase Report BronkopneumoniaBintang TrianaNessuna valutazione finora
- Myelodisplastic SyndromeDocumento9 pagineMyelodisplastic SyndromeEni JiantiNessuna valutazione finora
- Print PneumoniaDocumento24 paginePrint Pneumoniavandhani79Nessuna valutazione finora
- Demam TifoidDocumento106 pagineDemam TifoidMasYurahNharaBarusNessuna valutazione finora
- Typhoid Fever Case ReportDocumento32 pagineTyphoid Fever Case ReportAlvin PratamaNessuna valutazione finora
- Continuing Professional Development: The Role of Exogenous Surfactants in Treating Premature Infant Respiratory Distress SyndromeDocumento4 pagineContinuing Professional Development: The Role of Exogenous Surfactants in Treating Premature Infant Respiratory Distress Syndromelaudya100% (1)
- Lapsus Bangsal 1Documento20 pagineLapsus Bangsal 1Ira M RNessuna valutazione finora
- Tuberculous Meningitis Case ReportDocumento34 pagineTuberculous Meningitis Case ReportDippos Theofilus HNessuna valutazione finora
- Case Report Melita Aditya Sari 12-058Documento51 pagineCase Report Melita Aditya Sari 12-058Firda Diah UtamiNessuna valutazione finora
- Case Report Kejang DemamDocumento48 pagineCase Report Kejang DemamRahmatNessuna valutazione finora
- Case Report - Cutaneous Larva MigransDocumento15 pagineCase Report - Cutaneous Larva MigransDira Adhitya100% (1)
- Hypertension Treatment and GoalsDocumento41 pagineHypertension Treatment and GoalsSemestaNessuna valutazione finora
- Congenital GlaucomaDocumento27 pagineCongenital Glaucomaanon_373532435Nessuna valutazione finora
- Borang LohhDocumento22 pagineBorang LohhRezki RamadhanNessuna valutazione finora
- Otitis Media AkutDocumento31 pagineOtitis Media AkutNin DuskNessuna valutazione finora
- Abdominal Pain in Children - Dr. Hermanto SP - BaDocumento41 pagineAbdominal Pain in Children - Dr. Hermanto SP - Bajimmy_junNessuna valutazione finora
- MeningoencephalitisDocumento58 pagineMeningoencephalitisShillea Olimpia Melyta100% (1)
- Dr. Ago Harlim - MikosisDocumento50 pagineDr. Ago Harlim - MikosisBrian Pasa NababanNessuna valutazione finora
- Chronic Cephalgia and Hemiparese due to Brain TumorDocumento5 pagineChronic Cephalgia and Hemiparese due to Brain TumorrivienaNessuna valutazione finora
- Laporan Kasus CHFDocumento27 pagineLaporan Kasus CHFBerka Phillia NingrumNessuna valutazione finora
- Dermatological Infection Management UpdateDocumento29 pagineDermatological Infection Management UpdateyheyenNessuna valutazione finora
- Paederus Dermatitis Karthikeyan K, Kumar A - Indian J Dermatol Venereol LeprolDocumento11 paginePaederus Dermatitis Karthikeyan K, Kumar A - Indian J Dermatol Venereol Leprolalmas prawoto100% (1)
- Vitamin D Levels and Recurrent Tonsillitis in ChildrenDocumento14 pagineVitamin D Levels and Recurrent Tonsillitis in ChildrenMyarNessuna valutazione finora
- PPT Case NephrolithiasisDocumento45 paginePPT Case NephrolithiasisRifka Anisa0% (1)
- Trantornos Anorrectales Adquiridos PDFDocumento7 pagineTrantornos Anorrectales Adquiridos PDFIván Castellares RojasNessuna valutazione finora
- Kuliah TETANUSDocumento30 pagineKuliah TETANUSAraa AsukaNessuna valutazione finora
- Demam Tifoid: Etiologi, Gejala, Diagnosis dan PenatalaksanaanDocumento30 pagineDemam Tifoid: Etiologi, Gejala, Diagnosis dan PenatalaksanaanRaihan LuthfiNessuna valutazione finora
- Fix Case Report TifoidDocumento24 pagineFix Case Report Tifoidanggun nur auliaNessuna valutazione finora
- Pediatri Essensial 3Documento86 paginePediatri Essensial 3Gregorius WahyudiNessuna valutazione finora
- 10 - 258sepsis Neonatorum Awitan DiniDocumento4 pagine10 - 258sepsis Neonatorum Awitan DiniIrenaNessuna valutazione finora
- REFERAT - Meassles - FirdaDocumento19 pagineREFERAT - Meassles - FirdaEriza LuthfansyahNessuna valutazione finora
- Otitis MediaDocumento48 pagineOtitis MediaRaisah_Ridwan382Nessuna valutazione finora
- PertusisDocumento28 paginePertusiswenyinriantoNessuna valutazione finora
- Batu Saluran Kemih: Dr. Suhaemi, SPPD, FinasimDocumento57 pagineBatu Saluran Kemih: Dr. Suhaemi, SPPD, FinasimAfri AdiNessuna valutazione finora
- Sindrom Nefritik DebDocumento2 pagineSindrom Nefritik DebrchristevenNessuna valutazione finora
- Causes, Symptoms and Treatment of ChorioretinitisDocumento13 pagineCauses, Symptoms and Treatment of Chorioretinitisrada tri rosi kurniaNessuna valutazione finora
- Chorioretinitis: By. Bimo Nugroho SaktiDocumento14 pagineChorioretinitis: By. Bimo Nugroho SaktiSalman AlkomaNessuna valutazione finora
- Radiologi - Tambahan SsDocumento91 pagineRadiologi - Tambahan SsShifa TifarinNessuna valutazione finora
- Tutorial Kasus: AppendisitisDocumento50 pagineTutorial Kasus: Appendisitiseruza hiwatariNessuna valutazione finora
- Journal Reading THT - OMADocumento15 pagineJournal Reading THT - OMAIndira MaycellaNessuna valutazione finora
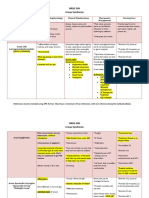
- NRSG 206 Croup SyndromeDocumento3 pagineNRSG 206 Croup SyndromeGirlwithnonameNessuna valutazione finora
- Pityriasis Rosea PatogenesisDocumento4 paginePityriasis Rosea PatogenesisAdrian KuswantoNessuna valutazione finora
- KERATITISDocumento12 pagineKERATITISfaridasylvia100% (1)
- Patient Medical RecordsDocumento50 paginePatient Medical Recordscamila anisNessuna valutazione finora
- Kista Ovarium 21906150Documento43 pagineKista Ovarium 21906150NUR ATHIFAHNessuna valutazione finora
- FIXED DRUG ERUPTION PrintDocumento17 pagineFIXED DRUG ERUPTION PrintnajwaNessuna valutazione finora
- Skull Cervical X-RayDocumento15 pagineSkull Cervical X-RayPuji Yunisyah RahayuNessuna valutazione finora
- PDF Borang Ukm Advokasi CompressDocumento8 paginePDF Borang Ukm Advokasi CompressJeffry HertantoNessuna valutazione finora
- Pneumonia in Children - Causes, Signs, SymptomsDocumento63 paginePneumonia in Children - Causes, Signs, SymptomsAbraham AnaelyNessuna valutazione finora
- Pneumonia Minggu GMEDocumento42 paginePneumonia Minggu GMEEkaNessuna valutazione finora
- Acquired PneumoniaeDocumento20 pagineAcquired PneumoniaeVivi DeviyanaNessuna valutazione finora
- Causes of Neonatal Pneumonia by Route - UpToDateDocumento2 pagineCauses of Neonatal Pneumonia by Route - UpToDateThảo Nguyên Phan NguyễnNessuna valutazione finora
- Bacteri Pathology&pathogenesisDocumento22 pagineBacteri Pathology&pathogenesisAsem AlhazmiNessuna valutazione finora
- Pneumonia Lobaris PneumoniaDocumento34 paginePneumonia Lobaris PneumoniamoditiaraNessuna valutazione finora
- HEAD INJURY (Trauma Kepala) DR - AgusDocumento53 pagineHEAD INJURY (Trauma Kepala) DR - AgusSetyo RahmanNessuna valutazione finora
- 11.2 Gas Exchange in Humans Igcse Cie Biology Ext Theory MsDocumento3 pagine11.2 Gas Exchange in Humans Igcse Cie Biology Ext Theory MsRyan NishadNessuna valutazione finora
- Anatomy ProstateDocumento2 pagineAnatomy ProstatenavjavNessuna valutazione finora
- How Pandemics Spread and WebquestDocumento3 pagineHow Pandemics Spread and Webquestapi-405140390Nessuna valutazione finora
- Chapter 4 Integumentary SystemDocumento75 pagineChapter 4 Integumentary SystemAngel JuNessuna valutazione finora
- Acid Base Balance and Arterial Blood Gas AnalysisDocumento29 pagineAcid Base Balance and Arterial Blood Gas AnalysisPaulus LukmanNessuna valutazione finora
- Pubic Health SurvilanceDocumento28 paginePubic Health Survilanceteklay100% (1)
- Sample Research Plan2Documento9 pagineSample Research Plan2api-283862617Nessuna valutazione finora
- Alteration in Endocrine SystemDocumento215 pagineAlteration in Endocrine Systemyen1988100% (1)
- A Stag God Is Born Ch6-7Documento12 pagineA Stag God Is Born Ch6-7Eka KimNessuna valutazione finora
- Question Paper Unit f214 Communication Homeostasis and EnergyDocumento16 pagineQuestion Paper Unit f214 Communication Homeostasis and EnergyRobert EdwardsNessuna valutazione finora
- Acadsoc BookDocumento6 pagineAcadsoc Bookmarizon datuNessuna valutazione finora
- Asphyxia by SuffocationDocumento15 pagineAsphyxia by SuffocationBryan Christopher Co Lao100% (1)
- Arun Kumar RayDocumento15 pagineArun Kumar RayAnil GautamNessuna valutazione finora
- 04 Bahas Inggris Paket 4Documento9 pagine04 Bahas Inggris Paket 4Aji PangestuNessuna valutazione finora
- CCGL 9061 PosterDocumento1 paginaCCGL 9061 Posterchunpan tsangNessuna valutazione finora
- Pathogens 11 00715 v2Documento25 paginePathogens 11 00715 v2Hizrah Harianto SembiringNessuna valutazione finora
- Blood LecturesDocumento128 pagineBlood LecturessrhrenaissanceNessuna valutazione finora
- Anti-FTO Antibody (EPR6894) Ab126605: 6 ImagesDocumento4 pagineAnti-FTO Antibody (EPR6894) Ab126605: 6 Imageshorace35Nessuna valutazione finora
- Thoracic Trauma TreatmentDocumento77 pagineThoracic Trauma TreatmentAnonymous GsvDOlQuSNessuna valutazione finora
- Gynaecological NursingDocumento79 pagineGynaecological NursingGuruKPO100% (3)
- Livestock Superviser Job Description JB SDDocumento2 pagineLivestock Superviser Job Description JB SDSkyNessuna valutazione finora
- Many Sides of RizalDocumento11 pagineMany Sides of Rizaljulieanntipon100% (1)
- Body Condition Score Dog PDFDocumento1 paginaBody Condition Score Dog PDFJairo Alfonso Angulo NegreteNessuna valutazione finora
- 9 Pengaruh Therapi Tertawa Terhadap Penurunan Tekanan Darah Pada Lansia Penderita Hipertensi Di PSTW Puspakarma Mataram Ni Made SumartyawatiDocumento2 pagine9 Pengaruh Therapi Tertawa Terhadap Penurunan Tekanan Darah Pada Lansia Penderita Hipertensi Di PSTW Puspakarma Mataram Ni Made Sumartyawatikadek aryaNessuna valutazione finora
- Marketing AttractionDocumento16 pagineMarketing AttractionIka DinNessuna valutazione finora
- Of TheDocumento81 pagineOf Theayushy gupta100% (1)
- NatokinaseDocumento6 pagineNatokinasefabadioNessuna valutazione finora
- MD Curs Neuro 4Documento45 pagineMD Curs Neuro 4Andreea AlexaNessuna valutazione finora
- Benign Ovarian ConditionsDocumento31 pagineBenign Ovarian ConditionsNur Hanani KhanNessuna valutazione finora