Potrebbero piacerti anche
- EpidemiologyDocumento33 pagineEpidemiologyBheru Lal100% (2)
- Epidemiology: Andre Bencee V. Barimbao, RMT, MLS (ASCP)Documento55 pagineEpidemiology: Andre Bencee V. Barimbao, RMT, MLS (ASCP)Alondra Aran100% (2)
- Basic Epidemiology (E-Book)Documento226 pagineBasic Epidemiology (E-Book)Ing Ching100% (12)
- Lecture Notes On EpidemiologyDocumento196 pagineLecture Notes On Epidemiologypushpa devkota100% (1)
- Epidemiology Lecture NotesDocumento178 pagineEpidemiology Lecture NotesImtiaz Husain83% (6)
- Principles of Epidemiology in Public Health PracticeDocumento512 paginePrinciples of Epidemiology in Public Health PracticeAdare Oluwafemi Thomas100% (3)
- Epidemiology and Demography in Public HealthDa EverandEpidemiology and Demography in Public HealthJaphet KillewoValutazione: 5 su 5 stelle5/5 (1)
- Introduction To Public HealthDocumento52 pagineIntroduction To Public Healthilatwins100% (4)
- DR Nazia Sultan Ali B.D.S., M.P.H. Senior Demonstrator Fatima Jinnah Dental CollegeDocumento100 pagineDR Nazia Sultan Ali B.D.S., M.P.H. Senior Demonstrator Fatima Jinnah Dental Collegestpd2dogs100% (1)
- Analytical EpidemiologyDocumento64 pagineAnalytical EpidemiologyQueency Dangilan100% (1)
- Epidemiology PPT NewDocumento100 pagineEpidemiology PPT NewSujatha Aluguri100% (2)
- Introduction To EpidemiologyDocumento117 pagineIntroduction To Epidemiologygbong19100% (2)
- Study Designs in Epidemiologic Research Chronic DiseasesDocumento51 pagineStudy Designs in Epidemiologic Research Chronic DiseasesLeonel Nkweti100% (2)
- Basic EpidemiologyDocumento28 pagineBasic Epidemiologybijugeorge1100% (2)
- Introduction To EpidemiologyDocumento87 pagineIntroduction To EpidemiologyMugisha Laurian100% (1)
- Text Book of Public Health and Community MedicineDocumento1.358 pagineText Book of Public Health and Community MedicineThomas Robert83% (40)
- Introduction To EpidemiologyDocumento39 pagineIntroduction To EpidemiologyAnn John100% (1)
- Epidemiology Principles and Methods Prof Bhisma MurtiDocumento32 pagineEpidemiology Principles and Methods Prof Bhisma Murtievy_silviania8873100% (1)
- Basic Measures of EpidemiologyDocumento51 pagineBasic Measures of EpidemiologyHafiz SabghatullahNessuna valutazione finora
- EpidemiologyDocumento86 pagineEpidemiologySainab Moohamoud83% (6)
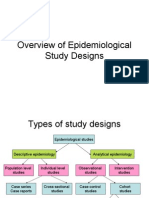
- Overview of Epidemiological Study DesignsDocumento16 pagineOverview of Epidemiological Study DesignsLakshmi Seth100% (2)
- Epidemiology MethodsDocumento481 pagineEpidemiology MethodsPippo KennedyNessuna valutazione finora
- Epidemiology 2Documento54 pagineEpidemiology 2oheneapeahrita100% (2)
- Epidemiology ReviewDocumento29 pagineEpidemiology Reviewjohnkad100% (4)
- EpidemiologyDocumento13 pagineEpidemiologyswethashaki50% (2)
- Epidemiology NotesDocumento16 pagineEpidemiology NotesAnonymous 1I0JCC96G2100% (1)
- 2 Epidemiology TerminologyDocumento33 pagine2 Epidemiology Terminologynithin shenoiNessuna valutazione finora
- Basics in Epidemiology & Biostatistics (2015) (PDF) (UnitedVRG)Documento192 pagineBasics in Epidemiology & Biostatistics (2015) (PDF) (UnitedVRG)Waleed Mostafa75% (4)
- An Introduction To Applied Epidemiology and BiostatisticsDocumento511 pagineAn Introduction To Applied Epidemiology and BiostatisticsMelissa Sindiong100% (7)
- Clinical Epidemiology 3rd EdDocumento283 pagineClinical Epidemiology 3rd Edkenz18096100% (3)
- Natural History of DiseaseDocumento26 pagineNatural History of Diseaseadinda mouzasNessuna valutazione finora
- Community MedicineDocumento6 pagineCommunity MedicineBee-joy Rana100% (1)
- Epidemiology: RD THDocumento21 pagineEpidemiology: RD THKailash Nagar100% (1)
- Epidemiology of Infectious DiseasesDocumento38 pagineEpidemiology of Infectious Diseasessarguss14100% (4)
- EpidemiologyDocumento40 pagineEpidemiologyCharityOchiengNessuna valutazione finora
- Basic Concepts of EpidemiologyDocumento125 pagineBasic Concepts of EpidemiologyKailash Nagar100% (1)
- Basic Concepts and Principles of EpidemiologyDocumento137 pagineBasic Concepts and Principles of EpidemiologyShubhamNessuna valutazione finora
- HTSC440 CH01Documento59 pagineHTSC440 CH01gypsy90Nessuna valutazione finora
- Introduction To Epidemiology Dr. Abdikani Ali MbbsDocumento38 pagineIntroduction To Epidemiology Dr. Abdikani Ali Mbbsabdikani hassanNessuna valutazione finora
- Introduction To EpidemiologyDocumento35 pagineIntroduction To EpidemiologyChipego NyirendaNessuna valutazione finora
- Introductiontoepidemiology 190213062350Documento45 pagineIntroductiontoepidemiology 190213062350Mangala bote Nair PSMNessuna valutazione finora
- Lecture 1 IntroductionDocumento27 pagineLecture 1 IntroductionEman KhammasNessuna valutazione finora
- What Is Epidemiology?Documento23 pagineWhat Is Epidemiology?KoushikNessuna valutazione finora
- Epidemiology Intro JayaDocumento39 pagineEpidemiology Intro JayajayalakshmiNessuna valutazione finora
- Aims of Epid LectureDocumento11 pagineAims of Epid LectureM7MD SHOWNessuna valutazione finora
- 1-Introduction MDDocumento38 pagine1-Introduction MDRasheena RasheeqNessuna valutazione finora
- Public Health CPH LectDocumento17 paginePublic Health CPH LectRosemarie QuibolNessuna valutazione finora
- Introduction To EpidemiologyDocumento15 pagineIntroduction To EpidemiologyNathnael Gebeyehu0% (1)
- Learning ObjectivesDocumento20 pagineLearning ObjectivesOmar MohamedNessuna valutazione finora
- Academic WritingDocumento48 pagineAcademic Writingسهى الغامديNessuna valutazione finora
- Epidemiology: Dr. Siswanto, M.SCDocumento65 pagineEpidemiology: Dr. Siswanto, M.SCSharan SekhonNessuna valutazione finora
- Introduction To EpidemiologyDocumento24 pagineIntroduction To EpidemiologyAstrid FausziaNessuna valutazione finora
- Principles of EpiDocumento29 paginePrinciples of Epirodelagapito100% (1)
- Introduction of EpiDocumento22 pagineIntroduction of Epidrrana.alshabiNessuna valutazione finora
- Epidemiology FinalDocumento90 pagineEpidemiology FinalMoumita hazarika100% (1)
- Epidermiology Unit 1Documento86 pagineEpidermiology Unit 1pushpa devkota100% (1)
- Public Health IDocumento78 paginePublic Health IHardik ParmarNessuna valutazione finora
- Epidemiology-I 2021 (STD Copy)Documento42 pagineEpidemiology-I 2021 (STD Copy)Poonam RanaNessuna valutazione finora
- Epidemiology: Chapter 1: IntroductionDocumento134 pagineEpidemiology: Chapter 1: IntroductionLoai Mohammed IssaNessuna valutazione finora
- Florance Nightingale Environmental TheoryDocumento54 pagineFlorance Nightingale Environmental TheoryKailash NagarNessuna valutazione finora
- Name of Regional Directorate of NSS-Ahmedabad State-GujaratDocumento9 pagineName of Regional Directorate of NSS-Ahmedabad State-GujaratKailash NagarNessuna valutazione finora
- Academic Bank of CreditDocumento13 pagineAcademic Bank of CreditKailash NagarNessuna valutazione finora
- 1604 - M.A. - M.sc. (Previous) Time Table-2021Documento18 pagine1604 - M.A. - M.sc. (Previous) Time Table-2021Kailash NagarNessuna valutazione finora
- MSC Program Academic Report 2020-21Documento34 pagineMSC Program Academic Report 2020-21Kailash NagarNessuna valutazione finora
- 2473-Article Text-3680-1-10-20210918Documento5 pagine2473-Article Text-3680-1-10-20210918Kailash NagarNessuna valutazione finora
- Second Year Post Basic B.SC NursingDocumento11 pagineSecond Year Post Basic B.SC NursingKailash Nagar100% (1)
- 03 Health Committees ReportsDocumento60 pagine03 Health Committees ReportsKailash NagarNessuna valutazione finora
- 04 HEALTH CARE DELIVERY SYSTEM INDIA For CHODocumento34 pagine04 HEALTH CARE DELIVERY SYSTEM INDIA For CHOKailash Nagar100% (1)
- Institute Name: University of Kota (IR-O-U-0387)Documento8 pagineInstitute Name: University of Kota (IR-O-U-0387)Kailash NagarNessuna valutazione finora
- 04 IPHS Primary Health CentreDocumento20 pagine04 IPHS Primary Health CentreKailash NagarNessuna valutazione finora
- 02 Historical Development of PHNDocumento32 pagine02 Historical Development of PHNKailash NagarNessuna valutazione finora
- Pricing Concepts,: Strategies and Price Setting ApproachesDocumento16 paginePricing Concepts,: Strategies and Price Setting ApproachesKailash NagarNessuna valutazione finora
- AEUP Application Form 1/5Documento5 pagineAEUP Application Form 1/5Kailash NagarNessuna valutazione finora
- Continuity in Indian AdministrationDocumento4 pagineContinuity in Indian AdministrationKailash NagarNessuna valutazione finora
- 01 Public Health NursingDocumento38 pagine01 Public Health NursingKailash NagarNessuna valutazione finora
- Poster For HelplineDocumento1 paginaPoster For HelplineKailash NagarNessuna valutazione finora
- AnganwadiDocumento8 pagineAnganwadiKailash NagarNessuna valutazione finora
- Ljnfyl"Vm Tyf Sd"Rfzlu6 Df8 (: LNGXF 58 (, SM, (H VMO GL "UDocumento1 paginaLjnfyl"Vm Tyf Sd"Rfzlu6 Df8 (: LNGXF 58 (, SM, (H VMO GL "UKailash NagarNessuna valutazione finora
- CHN Practical Procedure ListDocumento1 paginaCHN Practical Procedure ListKailash NagarNessuna valutazione finora
- Managing Product LinesDocumento10 pagineManaging Product LinesKailash NagarNessuna valutazione finora
- A Name, Term, Sign, Symbol or Design Intended To Identify The Goods or Services of A Seller and To Differentiate Them From CompetitionDocumento7 pagineA Name, Term, Sign, Symbol or Design Intended To Identify The Goods or Services of A Seller and To Differentiate Them From CompetitionKailash NagarNessuna valutazione finora
- 5 Marketing EnviromentDocumento21 pagine5 Marketing EnviromentKailash NagarNessuna valutazione finora
- Child Welfare AgenciesDocumento93 pagineChild Welfare AgenciesKailash Nagar80% (5)
- Fuzzy Gain Scheduled Pi Controller For ADocumento5 pagineFuzzy Gain Scheduled Pi Controller For AOumayNessuna valutazione finora
- Combined South Dakota Motions To Reconsider in ICWA CaseDocumento53 pagineCombined South Dakota Motions To Reconsider in ICWA CaseLee StranahanNessuna valutazione finora
- Coaxial Cable Attenuation ChartDocumento6 pagineCoaxial Cable Attenuation ChartNam PhamNessuna valutazione finora
- Genuine Fakes: How Phony Things Teach Us About Real StuffDocumento2 pagineGenuine Fakes: How Phony Things Teach Us About Real StuffGail LeondarWrightNessuna valutazione finora
- I M Com QT Final On16march2016Documento166 pagineI M Com QT Final On16march2016Khandaker Sakib Farhad0% (1)
- LP32HS User Manual v1Documento52 pagineLP32HS User Manual v1tonizx7rrNessuna valutazione finora
- 11.3.1 Some Special CasesDocumento10 pagine11.3.1 Some Special CasesSiddharth KishanNessuna valutazione finora
- WWW Studocu Com in N 29646569 Sid 01682568219Documento1 paginaWWW Studocu Com in N 29646569 Sid 01682568219Nivetha SelvamuruganNessuna valutazione finora
- How Chargers WorkDocumento21 pagineHow Chargers WorkMuhammad Irfan RiazNessuna valutazione finora
- Hockney-Falco Thesis: 1 Setup of The 2001 PublicationDocumento6 pagineHockney-Falco Thesis: 1 Setup of The 2001 PublicationKurayami ReijiNessuna valutazione finora
- Create A Visual DopplerDocumento1 paginaCreate A Visual DopplerRahul GandhiNessuna valutazione finora
- Analysis of Rates (Nh-15 Barmer - Sanchor)Documento118 pagineAnalysis of Rates (Nh-15 Barmer - Sanchor)rahulchauhan7869Nessuna valutazione finora
- Lesson 1 3 Transes in Reading in Philippine HistoryDocumento17 pagineLesson 1 3 Transes in Reading in Philippine HistoryNAPHTALI WILLIAMS GONessuna valutazione finora
- IT Level 4 COCDocumento2 pagineIT Level 4 COCfikru tesefaye0% (1)
- Pathogenic Escherichia Coli Associated With DiarrheaDocumento7 paginePathogenic Escherichia Coli Associated With DiarrheaSiti Fatimah RadNessuna valutazione finora
- Culture 2007 2013 Projects Overview 2018-03-18Documento133 pagineCulture 2007 2013 Projects Overview 2018-03-18PontesDeboraNessuna valutazione finora
- Sample REVISION QUESTION BANK. ACCA Paper F5 PERFORMANCE MANAGEMENTDocumento43 pagineSample REVISION QUESTION BANK. ACCA Paper F5 PERFORMANCE MANAGEMENTAbayneh Assefa75% (4)
- Ej. 1 Fin CorpDocumento3 pagineEj. 1 Fin CorpChantal AvilesNessuna valutazione finora
- Educationusa 2022globalguide Final Reduced SizeDocumento84 pagineEducationusa 2022globalguide Final Reduced SizeAnna ModebadzeNessuna valutazione finora
- MFE Module 1 .Documento15 pagineMFE Module 1 .Adarsh KNessuna valutazione finora
- CISF Manual Final OriginalDocumento17 pagineCISF Manual Final OriginalVaishnavi JayakumarNessuna valutazione finora
- Lacey Robertson Resume 3-6-20Documento1 paginaLacey Robertson Resume 3-6-20api-410771996Nessuna valutazione finora
- Alfa Week 1Documento13 pagineAlfa Week 1Cikgu kannaNessuna valutazione finora
- Mission and VisionDocumento5 pagineMission and VisionsanjedNessuna valutazione finora
- Trina 440W Vertex-S+ DatasheetDocumento2 pagineTrina 440W Vertex-S+ DatasheetBrad MannNessuna valutazione finora
- 25 Middlegame Concepts Every Chess Player Must KnowDocumento2 pagine25 Middlegame Concepts Every Chess Player Must KnowKasparicoNessuna valutazione finora
- Day6 7Documento11 pagineDay6 7Abu Al-FarouqNessuna valutazione finora
- Grade 8 Science - Second GradingDocumento5 pagineGrade 8 Science - Second GradingMykelCañete0% (1)
- Maya Deren PaperDocumento9 pagineMaya Deren PaperquietinstrumentalsNessuna valutazione finora
- CHARACTER FORMATION 1 PrelimDocumento15 pagineCHARACTER FORMATION 1 PrelimAiza Minalabag100% (1)