Potrebbero piacerti anche
- A New Concept of ShockDocumento52 pagineA New Concept of ShockKADEK ARTAWANNessuna valutazione finora
- Acute Life Threatening Events ManagementDocumento58 pagineAcute Life Threatening Events ManagementFebe Sintia KristianiNessuna valutazione finora
- Manajemen Shock Pada AnakDocumento71 pagineManajemen Shock Pada AnakmentariyuhendarNessuna valutazione finora
- Dr. Bastian - ShockDocumento44 pagineDr. Bastian - ShockKARDIOLOGI STASE RSALNessuna valutazione finora
- IV Fluid Therapy GuideDocumento81 pagineIV Fluid Therapy GuideMarsa ZaidanNessuna valutazione finora
- Malignant Hyperthermia: Barbara Robertson, MD, FRCPC Dept of Anesthesia, PAHDocumento34 pagineMalignant Hyperthermia: Barbara Robertson, MD, FRCPC Dept of Anesthesia, PAHLee Chee SengNessuna valutazione finora
- Spontaneos Breathing TrialsDocumento16 pagineSpontaneos Breathing Trialsjohnmaster2010Nessuna valutazione finora
- Allergic PDFDocumento17 pagineAllergic PDFSiska HarapanNessuna valutazione finora
- Chapter 4 Florence Nightingales Legacy of Caring and Its Applications 1Documento23 pagineChapter 4 Florence Nightingales Legacy of Caring and Its Applications 1api-308551668Nessuna valutazione finora
- Code Stroke Emergency ResponseDocumento35 pagineCode Stroke Emergency Responsedewi wijayantiNessuna valutazione finora
- Diagnosis Dan Tatalaksana Syok Di Layanan Primer: Rs Pratama Teluk KeramatDocumento45 pagineDiagnosis Dan Tatalaksana Syok Di Layanan Primer: Rs Pratama Teluk KeramatNight BaronNessuna valutazione finora
- Telaah Kritis Disain Penelitian KualitatifDocumento16 pagineTelaah Kritis Disain Penelitian KualitatifAnonymous Au0vHUNessuna valutazione finora
- Konas Perdatin 2019Documento66 pagineKonas Perdatin 2019Akreditasi RSPC19Nessuna valutazione finora
- PHBS, 7 Cara Meningkatkan Kesehatan KeluargaDocumento2 paginePHBS, 7 Cara Meningkatkan Kesehatan KeluargaYeny Endang EndongNessuna valutazione finora
- Terapi OksigenDocumento12 pagineTerapi OksigenYohana SepthiyaNessuna valutazione finora
- Acute Miocard InfarkDocumento32 pagineAcute Miocard InfarkhansNessuna valutazione finora
- Intisari Peranan Teknologi Perikanan Untuk Menunjang Perekonomian NasionalDocumento7 pagineIntisari Peranan Teknologi Perikanan Untuk Menunjang Perekonomian NasionalJurnal Agroforestry100% (1)
- Epilepsi (Repaired) FixDocumento28 pagineEpilepsi (Repaired) FixNodya Wijaya Kusuma MaharaniNessuna valutazione finora
- Anestesi LaparoskopiDocumento65 pagineAnestesi LaparoskopiArief Hariyadi SantosoNessuna valutazione finora
- Analgesi Dan Sedasi Di IcuDocumento32 pagineAnalgesi Dan Sedasi Di IcuWidi Yuli HariantoNessuna valutazione finora
- Malaysiantriagescalenewrevised2019!1!221014090642 28d8e1aeDocumento18 pagineMalaysiantriagescalenewrevised2019!1!221014090642 28d8e1aenaqibsakila4286Nessuna valutazione finora
- SsDocumento11 pagineSsIrna MegawatyNessuna valutazione finora
- Trombosis Vena Dalam: Pendidikan Kedokteran Berkelanjutan (PKB) XXI 2013Documento13 pagineTrombosis Vena Dalam: Pendidikan Kedokteran Berkelanjutan (PKB) XXI 2013IkaNessuna valutazione finora
- Dr. Navy - Basic & Initial Setting 1Documento70 pagineDr. Navy - Basic & Initial Setting 1Ida KatarinaNessuna valutazione finora
- Stewart and Buffer Base.Documento69 pagineStewart and Buffer Base.Yohanes George100% (1)
- Shouldice HospitalDocumento8 pagineShouldice Hospitalvaishnavi subramanianNessuna valutazione finora
- Makalah Bahasa Inggris (Jantung)Documento12 pagineMakalah Bahasa Inggris (Jantung)Nia Mldyni100% (1)
- Vasoactive TherapyDocumento26 pagineVasoactive Therapylidya agustinNessuna valutazione finora
- Biodata Parestesi Juli 2011 Edit Ipo ++Documento55 pagineBiodata Parestesi Juli 2011 Edit Ipo ++rahmat feryadi0% (1)
- 2016 PAD ACC+AHA SlidesDocumento74 pagine2016 PAD ACC+AHA SlidesPonpimol Odee BongkeawNessuna valutazione finora
- Ventilator Weaning and Spontaneous Breathing Trials An Educational Review 2016Documento7 pagineVentilator Weaning and Spontaneous Breathing Trials An Educational Review 2016Tarran PhagooNessuna valutazione finora
- Essential First Aid SkillsDocumento17 pagineEssential First Aid SkillsMary Ann VALLECERNessuna valutazione finora
- Pemeriksaan Foto Thorax Pada Anak-AnakDocumento29 paginePemeriksaan Foto Thorax Pada Anak-AnakRenaldy PamungkasNessuna valutazione finora
- DIABETIC ULCER COMPLEXITIES AND MANAGEMENTDocumento56 pagineDIABETIC ULCER COMPLEXITIES AND MANAGEMENTmucfhsinNessuna valutazione finora
- Extubation Criteria & Delayed EmergenceDocumento3 pagineExtubation Criteria & Delayed EmergenceAnonymous OlS0WZwNessuna valutazione finora
- Bedah 1Documento20 pagineBedah 1ulfaNessuna valutazione finora
- Labioschizis Dan Palatoskisis Persentasi Kelompok 1Documento17 pagineLabioschizis Dan Palatoskisis Persentasi Kelompok 1Hengky HanggaraNessuna valutazione finora
- Guideline Sepsis TerbaruDocumento81 pagineGuideline Sepsis TerbaruasepNessuna valutazione finora
- Hemiballismus Is A Very Rare Movement DisorderDocumento5 pagineHemiballismus Is A Very Rare Movement Disorderapi-19973386Nessuna valutazione finora
- Dr. Mirza Koeshardiandi ABC of BurnDocumento35 pagineDr. Mirza Koeshardiandi ABC of Burnagus susantoNessuna valutazione finora
- Complications of Tuberculosis Review 2014Documento8 pagineComplications of Tuberculosis Review 2014EddyNessuna valutazione finora
- Case Study Peran Teori Keperawatan PDFDocumento5 pagineCase Study Peran Teori Keperawatan PDFLayung SariNessuna valutazione finora
- Management of Hypoxia During AnaesthesiaDocumento5 pagineManagement of Hypoxia During AnaesthesiaNurhafizahImfista100% (1)
- Tatalaksana Awal Koreksi Cairan pada Kasus SyokDocumento60 pagineTatalaksana Awal Koreksi Cairan pada Kasus Syokmuhammad benyNessuna valutazione finora
- II. Modul 5 - Terapi OksigenDocumento81 pagineII. Modul 5 - Terapi OksigenPerisha VeeraNessuna valutazione finora
- Antibiotic Evaluation in CAP Therapy at Budi Asih HospitalDocumento5 pagineAntibiotic Evaluation in CAP Therapy at Budi Asih HospitalKoko NugrohoNessuna valutazione finora
- Why Patient Safety Is Relevant To Surgery and Invasive ProceduresDocumento13 pagineWhy Patient Safety Is Relevant To Surgery and Invasive ProceduresNasriah DamayanthieNessuna valutazione finora
- Farmakologi Obat Analgesik, Anti Piretik & Anti Inflamasi: Andri Tilaqza, M.Farm., AptDocumento45 pagineFarmakologi Obat Analgesik, Anti Piretik & Anti Inflamasi: Andri Tilaqza, M.Farm., AptDark BlueNessuna valutazione finora
- Patient Centred Clinical MethodDocumento4 paginePatient Centred Clinical MethodSanita BNessuna valutazione finora
- Mengenal Resusitasi Pada Anak Dan Bayi Bagi Perawat PemulaDocumento15 pagineMengenal Resusitasi Pada Anak Dan Bayi Bagi Perawat PemulaSiti Krisan WijayaNessuna valutazione finora
- Ketoasidosis Diabetikum DAN Status Hiperosmolar HiperglikemikDocumento18 pagineKetoasidosis Diabetikum DAN Status Hiperosmolar HiperglikemikHaha RowlingNessuna valutazione finora
- Preskas Hypoxic Spell Patofisiologi Dan ManajemenDocumento22 paginePreskas Hypoxic Spell Patofisiologi Dan Manajemensurya marthiasNessuna valutazione finora
- Pemeriksaan Tanda Vital-Kuliah PengantarDocumento22 paginePemeriksaan Tanda Vital-Kuliah PengantarDwitia IswariNessuna valutazione finora
- Hubungan Pola Merokok Dengan Kejadian AsmaDocumento11 pagineHubungan Pola Merokok Dengan Kejadian AsmaLivilia MiftaNessuna valutazione finora
- B.1 Applied Anatomy of Thorax - Asisten 2015 2Documento126 pagineB.1 Applied Anatomy of Thorax - Asisten 2015 2Stefany FanyNessuna valutazione finora
- Farmakologi Penyakit-Penyakit Degenerasi Tulang Dan SendiDocumento19 pagineFarmakologi Penyakit-Penyakit Degenerasi Tulang Dan SendiCici MastaNessuna valutazione finora
- Airway EquipmentDocumento47 pagineAirway Equipmentyoustiana dwi rusitaNessuna valutazione finora
- Laporan KasusDocumento20 pagineLaporan KasusaryaNessuna valutazione finora
- Terapi PaliatifDocumento46 pagineTerapi PaliatifViviViviNessuna valutazione finora
- Oxygen Delivery: Franz Josef TariganDocumento57 pagineOxygen Delivery: Franz Josef TariganFranz TariganNessuna valutazione finora
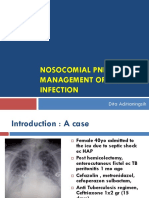
- MANAGE NOSOCOMIAL PNEUMONIADocumento64 pagineMANAGE NOSOCOMIAL PNEUMONIAAnggara DwiputraNessuna valutazione finora
- Antibiotik Pada Pasien Sakit Kritis: Adhrie Sugiarto FKUI / RSUPN Cipto Mangunkusumo Jakarta 2014Documento25 pagineAntibiotik Pada Pasien Sakit Kritis: Adhrie Sugiarto FKUI / RSUPN Cipto Mangunkusumo Jakarta 2014Anggara DwiputraNessuna valutazione finora
- Antibiotik Pada Pasien Sakit Kritis: Adhrie Sugiarto FKUI / RSUPN Cipto Mangunkusumo Jakarta 2014Documento25 pagineAntibiotik Pada Pasien Sakit Kritis: Adhrie Sugiarto FKUI / RSUPN Cipto Mangunkusumo Jakarta 2014Anggara DwiputraNessuna valutazione finora
- Berapa Nilai Parameter Hemodinamik Utk. Diagnosis PH?Documento58 pagineBerapa Nilai Parameter Hemodinamik Utk. Diagnosis PH?Anggara DwiputraNessuna valutazione finora
- Miranda Sings QuotesDocumento13 pagineMiranda Sings Quoteskarategirl201Nessuna valutazione finora
- Cousins Cum 4 1Documento15 pagineCousins Cum 4 1ty.mcgillNessuna valutazione finora
- The Teachings of DiogenesDocumento14 pagineThe Teachings of Diogenesryanash777100% (1)
- R-Controlled VowelsDocumento10 pagineR-Controlled VowelsShelby BruzzeseNessuna valutazione finora
- Ancient Greek Myths and Their OriginsDocumento28 pagineAncient Greek Myths and Their OriginsJenny WoychukNessuna valutazione finora
- Tissue Eng ToolsDocumento20 pagineTissue Eng ToolsVijay RajNessuna valutazione finora
- Sporák Instalace A Pou Ití: Cooker Installation and Use Konyhabútor Beépítés És HasználatDocumento44 pagineSporák Instalace A Pou Ití: Cooker Installation and Use Konyhabútor Beépítés És HasználatZbarl33chNessuna valutazione finora
- Concept Map - Abby !Documento2 pagineConcept Map - Abby !Abegail Abaygar100% (3)
- Practical Ent AbridgedDocumento17 paginePractical Ent AbridgedAishaNessuna valutazione finora
- ProverbDocumento38 pagineProverbAnkita GoelNessuna valutazione finora
- Ashes Reborn - WikiDocumento27 pagineAshes Reborn - WikiIvan StancheffNessuna valutazione finora
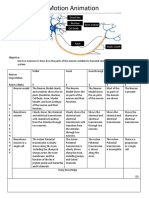
- Neurons Stop Motion AnimationDocumento2 pagineNeurons Stop Motion Animationapi-495006167Nessuna valutazione finora
- Vence Ferrell - The Vaccination CrisisDocumento177 pagineVence Ferrell - The Vaccination CrisisIna Hasim100% (1)
- American ConsonantsDocumento22 pagineAmerican ConsonantsAllanSalardaAdemNessuna valutazione finora
- Advances in Understanding The Urine-Concentrating MechanismDocumento26 pagineAdvances in Understanding The Urine-Concentrating MechanismKiara Lopez RelaizaNessuna valutazione finora
- Creative ParkDocumento14 pagineCreative ParkAli SimsekNessuna valutazione finora
- How To Clicker Train Your Cat PDFDocumento5 pagineHow To Clicker Train Your Cat PDFNesly100% (1)
- The Five-Minute Daily Energy RoutineDocumento4 pagineThe Five-Minute Daily Energy RoutineSatinder Bhalla100% (1)
- Lymphoid System Organs and Cells ExplainedDocumento31 pagineLymphoid System Organs and Cells ExplainedMace DueñasNessuna valutazione finora
- Erwin Straus Upright PostureDocumento33 pagineErwin Straus Upright PostureDem OsthenesNessuna valutazione finora
- Rapid Assessment SheetDocumento5 pagineRapid Assessment SheetElise HowardNessuna valutazione finora
- Life Sciences P2 Nov 2010 EngDocumento14 pagineLife Sciences P2 Nov 2010 Engbellydanceafrica9540Nessuna valutazione finora
- T4ADocumento2 pagineT4Ageorgianam992064Nessuna valutazione finora
- Paed HistDocumento123 paginePaed HistG VenkateshNessuna valutazione finora
- Anatomical TermsDocumento8 pagineAnatomical TermsDAGUMAN, FIONA DEI L.Nessuna valutazione finora
- 866349-Harrowspire Print FriendlyDocumento30 pagine866349-Harrowspire Print FriendlyCristian Jimenez0% (1)
- Status of Poultry Industry in Sri LankaDocumento21 pagineStatus of Poultry Industry in Sri LankaDickson MahanamaNessuna valutazione finora
- Mage The Awakening - Intruders - Encounters With The Abyss PDFDocumento228 pagineMage The Awakening - Intruders - Encounters With The Abyss PDFJohnRichardWuethrich100% (2)
- Reading and Wrting Performance TaskDocumento13 pagineReading and Wrting Performance TaskjefeljoevillacortaNessuna valutazione finora
- LearnEnglish ProfessionalsPodcasts Biotechnology 0Documento3 pagineLearnEnglish ProfessionalsPodcasts Biotechnology 0dinaria_ruNessuna valutazione finora