Potrebbero piacerti anche
- Wanita 18 Tahun Dengan Peritonitis TB Dan Tuberculosis Paru Kasus Baru Bta PositifDocumento20 pagineWanita 18 Tahun Dengan Peritonitis TB Dan Tuberculosis Paru Kasus Baru Bta PositifNur IndayantiNessuna valutazione finora
- Carcinoma Rectum - Janak - NEWDocumento74 pagineCarcinoma Rectum - Janak - NEWTowhidulIslamNessuna valutazione finora
- Ukuran PneumothoraxDocumento3 pagineUkuran PneumothoraxsultantraNessuna valutazione finora
- Respiratory System DisordersDocumento115 pagineRespiratory System DisordersFaith Levi Alecha Alferez100% (1)
- Jurnal Edema ParuDocumento54 pagineJurnal Edema Paruindah sariNessuna valutazione finora
- Anatomy and Physiology of The Respiratory SystemDocumento4 pagineAnatomy and Physiology of The Respiratory SystemchacameroNessuna valutazione finora
- SCHOOL COPY Gen Bio 1 - Q2 Module 4Documento20 pagineSCHOOL COPY Gen Bio 1 - Q2 Module 4PLS help me get 1k subsNessuna valutazione finora
- Restrictive Lung DiseasesDocumento31 pagineRestrictive Lung DiseasesAnn FrancisNessuna valutazione finora
- Mechanical VentilationDocumento43 pagineMechanical VentilationdesikristiyantiNessuna valutazione finora
- Mechanical VentilationDocumento43 pagineMechanical VentilationdesikristiyantiNessuna valutazione finora
- Atelektasis: Penyaji: Martvera SDocumento20 pagineAtelektasis: Penyaji: Martvera Saidil ilham100% (1)
- DLL (Science 9, Module 1, Unit 1, Week 1)Documento4 pagineDLL (Science 9, Module 1, Unit 1, Week 1)liberty100% (10)
- Respiration 1 MCQ 12 Nos With Key PDFDocumento8 pagineRespiration 1 MCQ 12 Nos With Key PDFAnonymous fn9zdHU7100% (3)
- NCM 112 - Practice TestDocumento6 pagineNCM 112 - Practice TestUzumaki K100% (1)
- Grade 9 Respiratory SystemDocumento22 pagineGrade 9 Respiratory SystemChristine Gacula100% (1)
- Alterations in Respiratory FunctionsDocumento26 pagineAlterations in Respiratory FunctionsAjeeshNessuna valutazione finora
- Empyema and Chest Tube - Dr. Gama SatriaDocumento28 pagineEmpyema and Chest Tube - Dr. Gama SatriaGresham Arceliusindi MulyaNessuna valutazione finora
- Monitoring Intra Operatif: Mindi Widayani NRP 122.022.1115 FK UPN "Veteran" JakartaDocumento21 pagineMonitoring Intra Operatif: Mindi Widayani NRP 122.022.1115 FK UPN "Veteran" Jakartaputri wulandariNessuna valutazione finora
- Hemorrhoid: Arief Aulia Rahman Pembimbing: Dr. Hj. Yanti Daryanti, SP.B-KBDDocumento35 pagineHemorrhoid: Arief Aulia Rahman Pembimbing: Dr. Hj. Yanti Daryanti, SP.B-KBDaryaharishalNessuna valutazione finora
- Chest TubeDocumento8 pagineChest TubeTaufik Nur YahyaNessuna valutazione finora
- Polycythemia Vera: Nurmaratu Thahirah Suaib C014172174Documento12 paginePolycythemia Vera: Nurmaratu Thahirah Suaib C014172174amiraNessuna valutazione finora
- CSS Airway Management RickyDocumento53 pagineCSS Airway Management RickyArtha PutuNessuna valutazione finora
- Practical Applications of Mechanical Ventilation PDFDocumento574 paginePractical Applications of Mechanical Ventilation PDFmladja77Nessuna valutazione finora
- Chest Tube InsertionDocumento36 pagineChest Tube InsertionskripsianiNessuna valutazione finora
- Hypoxia: Syafira Nurfitri 1501211054Documento14 pagineHypoxia: Syafira Nurfitri 1501211054Agnes Nina EurekaNessuna valutazione finora
- Hemangiomas, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandHemangiomas, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Acute Pulmonary Edema - NEJMDocumento4 pagineAcute Pulmonary Edema - NEJMSuzika Dewi0% (1)
- Tehnik - Tehnik Analgesia Post OperasiDocumento32 pagineTehnik - Tehnik Analgesia Post OperasiGuntur Aryo PuntodewoNessuna valutazione finora
- Ventricular Septal Defect: Present by Nur Kurnia Putri Halim Supervisor Dr. Akhtar Fajar M, SPJP, FihaDocumento31 pagineVentricular Septal Defect: Present by Nur Kurnia Putri Halim Supervisor Dr. Akhtar Fajar M, SPJP, FihaChintya Fidelia MontangNessuna valutazione finora
- Referat RahmanDocumento27 pagineReferat Rahmannasution7Nessuna valutazione finora
- PVC Stoelting Coex 1Documento29 paginePVC Stoelting Coex 1Rudy SiahaanNessuna valutazione finora
- AnestesiDocumento59 pagineAnestesiJeffrey EkaNessuna valutazione finora
- Refrst Sindrom KompartementDocumento28 pagineRefrst Sindrom Kompartementdesti cahyantiNessuna valutazione finora
- Wound de His Cence FinalDocumento26 pagineWound de His Cence Finaldanil armandNessuna valutazione finora
- Journal Reading Kista BartolinDocumento16 pagineJournal Reading Kista BartolinAnnisa SaragiNessuna valutazione finora
- Drug EruptionDocumento46 pagineDrug EruptionSyahDikaNessuna valutazione finora
- Responsi Spontan PneumothoraxDocumento49 pagineResponsi Spontan PneumothoraxNizarAbdullahNessuna valutazione finora
- Hernia: Rosaline Nike Sairlela 11.2013.024Documento37 pagineHernia: Rosaline Nike Sairlela 11.2013.024siscahildaNessuna valutazione finora
- KARSINOMA TIROID ZakiDocumento31 pagineKARSINOMA TIROID ZakiDenny LukasNessuna valutazione finora
- Metastasis Bone DiseaseDocumento11 pagineMetastasis Bone DiseasedrkurniatiNessuna valutazione finora
- Usg ThoraxDocumento64 pagineUsg ThoraxArvind KanagaratnamNessuna valutazione finora
- Hernia: and Other Digestive Congenital DiseaseDocumento14 pagineHernia: and Other Digestive Congenital DiseaseLingga GumelarNessuna valutazione finora
- Referat Tumor MamaeDocumento29 pagineReferat Tumor MamaefuadaffanNessuna valutazione finora
- Torsio Testis2016Documento6 pagineTorsio Testis2016Patrico Rillah SetiawanNessuna valutazione finora
- Cara Mengukur Tekanan IntrakompartemenDocumento2 pagineCara Mengukur Tekanan Intrakompartemenfatimah putriNessuna valutazione finora
- MediastinumDocumento27 pagineMediastinumAndrei PanaNessuna valutazione finora
- Edh, SDH, & Burr HolesDocumento46 pagineEdh, SDH, & Burr HolesRully Riyan DikaNessuna valutazione finora
- Healthcare Associated Pneumonia - Dr. Christian A. Johannes, SP - an.KICDocumento30 pagineHealthcare Associated Pneumonia - Dr. Christian A. Johannes, SP - an.KICvenyNessuna valutazione finora
- ASMADocumento61 pagineASMAdinimusman100% (1)
- Acute Urinary Retention: Ronald TanggoDocumento63 pagineAcute Urinary Retention: Ronald TanggoKalista ApriyaniNessuna valutazione finora
- 3.trauma Vaskular Richard SDocumento79 pagine3.trauma Vaskular Richard SAdang SunandarNessuna valutazione finora
- Referat HemothoraksDocumento28 pagineReferat HemothoraksitsmediNessuna valutazione finora
- Eloesser Flap Thoracostomy WindowDocumento20 pagineEloesser Flap Thoracostomy WindowJEFFRI JEFFRINessuna valutazione finora
- ROZERPLASTYDocumento13 pagineROZERPLASTYSaraya AmajidaNessuna valutazione finora
- 194 Surgical Cases PDFDocumento160 pagine194 Surgical Cases PDFkint100% (4)
- Critical Limb IschemiaDocumento11 pagineCritical Limb Ischemianurliah armandNessuna valutazione finora
- CR DR - Dedi Hidropneumothorax Ec TB ParuDocumento38 pagineCR DR - Dedi Hidropneumothorax Ec TB ParuBunga Listia ParamitaNessuna valutazione finora
- Referat Kandidosis Kutis - Dhira Dan A. Fari-70700120034 Dan 038Documento14 pagineReferat Kandidosis Kutis - Dhira Dan A. Fari-70700120034 Dan 038Ahmad Fari Arief LopaNessuna valutazione finora
- Skin GraftDocumento38 pagineSkin GraftAndika August100% (1)
- Fibroadenoma Mammae of The BreastDocumento15 pagineFibroadenoma Mammae of The Breastirvanie100% (1)
- Cervical Spine InjuriesDocumento18 pagineCervical Spine InjuriesAnnapurna DangetiNessuna valutazione finora
- Operative ObstetricsDocumento6 pagineOperative ObstetricsGrasya ZackieNessuna valutazione finora
- Acute AbdomenDocumento42 pagineAcute AbdomenErika Agustina KasdjonoNessuna valutazione finora
- Referat Kulit KakayDocumento26 pagineReferat Kulit KakayRezky Dwiputra FellanysNessuna valutazione finora
- (POIN) To Prediksi 1-50 Batch 2 2018 (Poinpoin)Documento344 pagine(POIN) To Prediksi 1-50 Batch 2 2018 (Poinpoin)Andika ZuldiansyahNessuna valutazione finora
- ThoracostomyDocumento10 pagineThoracostomywabalyNessuna valutazione finora
- Anatomi, Eflouresensi KulitDocumento67 pagineAnatomi, Eflouresensi KulitWhydia Wedha SutedjaNessuna valutazione finora
- Tinjauan Pustaka Rehabilitasi Medik Pada Pasien Geriatriulkus DecubitusDocumento6 pagineTinjauan Pustaka Rehabilitasi Medik Pada Pasien Geriatriulkus Decubitusrinaldy prayudhiaNessuna valutazione finora
- Retinopati DiabetikDocumento5 pagineRetinopati DiabetikMuhammad Afriadi HamdanNessuna valutazione finora
- Resusitasi NeonatusDocumento22 pagineResusitasi NeonatusnikkitaihsanNessuna valutazione finora
- EMPYEMADocumento27 pagineEMPYEMAMark Bin S. DilangalenNessuna valutazione finora
- Dermatoscopy and Skin Cancer, updated edition: A handbook for hunters of skin cancer and melanomaDa EverandDermatoscopy and Skin Cancer, updated edition: A handbook for hunters of skin cancer and melanomaNessuna valutazione finora
- Ineffective Airway ClearanceDocumento9 pagineIneffective Airway ClearanceMarissa AsimNessuna valutazione finora
- Pink Puffer Blue BloaterDocumento10 paginePink Puffer Blue BloaterMelinda MarianniNessuna valutazione finora
- Topic 1 - Pulmonary Anatomy, Physiology and Assessment (Hemo)Documento39 pagineTopic 1 - Pulmonary Anatomy, Physiology and Assessment (Hemo)Ben JilhanoNessuna valutazione finora
- Rebreather Design Optimizing Pendulum TypesDocumento7 pagineRebreather Design Optimizing Pendulum TypesSusan ColemanNessuna valutazione finora
- Arterial Blood Gases and Oxygen Content in Climbers On Mount EverestDocumento10 pagineArterial Blood Gases and Oxygen Content in Climbers On Mount EveresthendersonNessuna valutazione finora
- Impaired Gas ExchangeDocumento3 pagineImpaired Gas ExchangePaul VincentNessuna valutazione finora
- Closed Vs Open SuctionDocumento5 pagineClosed Vs Open SuctionKhushboo DurejaNessuna valutazione finora
- Fabian 2Documento6 pagineFabian 2przy3_14Nessuna valutazione finora
- ARDSDocumento6 pagineARDSarcobaleno589Nessuna valutazione finora
- Respiratory System 1 Physiology 16-11-2018Documento25 pagineRespiratory System 1 Physiology 16-11-2018Kangwa MasekaNessuna valutazione finora
- Should Fev1 Be Used To Grade Restrictive Impairment A Single Center Comparison of Lung Function Parameters To 6 Minute Walk Test in Patients With Restrictive Lung DiseaseDocumento5 pagineShould Fev1 Be Used To Grade Restrictive Impairment A Single Center Comparison of Lung Function Parameters To 6 Minute Walk Test in Patients With Restrictive Lung DiseaseHerald Scholarly Open AccessNessuna valutazione finora
- Terapi Oksigen KPPIKDocumento42 pagineTerapi Oksigen KPPIKAtikah PurnamasariNessuna valutazione finora
- Unit 7 - Respiratory SystemDocumento51 pagineUnit 7 - Respiratory SystemAbdullah MohammedNessuna valutazione finora
- Unit 4: Cellular Respiration Unit PlanDocumento3 pagineUnit 4: Cellular Respiration Unit Planapi-323720899Nessuna valutazione finora
- Lesson-9 1Documento26 pagineLesson-9 1Aihk kenneth BaronaNessuna valutazione finora
- Hypoxia SeminarDocumento18 pagineHypoxia Seminarmkyg4k4xwtNessuna valutazione finora
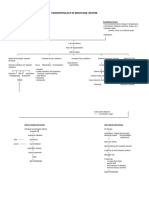
- Pathophysiology of Bronchial AsthmaDocumento2 paginePathophysiology of Bronchial AsthmaCarlos NiñoNessuna valutazione finora
- Respiratory SystemDocumento12 pagineRespiratory SystemHema Kamat100% (1)