Potrebbero piacerti anche
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5795)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1091)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- VertigoDocumento41 pagineVertigoAnonymous 4Oe8clFY100% (1)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Treatment Resistance in Psychiatry - Risk Factors, Biology, and Management-Springer Singapore (2019) PDFDocumento415 pagineTreatment Resistance in Psychiatry - Risk Factors, Biology, and Management-Springer Singapore (2019) PDFDrAvik Chakraborty100% (1)
- Saudi Board Question Bank PDFDocumento414 pagineSaudi Board Question Bank PDFbwaey100% (2)
- Clinical Log Book BSC Nursing 170622Documento87 pagineClinical Log Book BSC Nursing 170622Shital Pawar100% (1)
- NUMC 101B Endocrine System Laboratory ExerciseDocumento17 pagineNUMC 101B Endocrine System Laboratory ExerciseMelody Boado100% (1)
- NTCP TCPDocumento54 pagineNTCP TCPSAlonii Chawla100% (2)
- What Are Electrolytes? What Causes Electrolyte Imbalance?: Fast Facts On ElectrolytesDocumento11 pagineWhat Are Electrolytes? What Causes Electrolyte Imbalance?: Fast Facts On ElectrolytesL InfiniteNessuna valutazione finora
- Icru 38-Dose, Volume and Reporting Intracavitary Brachytherapy in GynDocumento25 pagineIcru 38-Dose, Volume and Reporting Intracavitary Brachytherapy in GynSAlonii ChawlaNessuna valutazione finora
- Construction, Design and Comissioning of MLC ForDocumento74 pagineConstruction, Design and Comissioning of MLC ForSAlonii ChawlaNessuna valutazione finora
- Drug Study - Hepatitis B VaccineDocumento2 pagineDrug Study - Hepatitis B VaccineJustin AncogNessuna valutazione finora
- Icru 38Documento33 pagineIcru 38SAlonii ChawlaNessuna valutazione finora
- Nursing Department: Answer: RationaleDocumento14 pagineNursing Department: Answer: RationaleEsmareldah Henry SirueNessuna valutazione finora
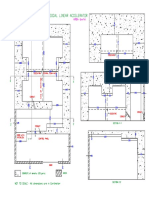
- Typical Layout of 15mv Medical Linear AcceleratorDocumento1 paginaTypical Layout of 15mv Medical Linear AcceleratorSAlonii ChawlaNessuna valutazione finora
- Trs 398 Protocol For Photons: Moderator: Mrs. Reena Sharma Presented By: Parikshit SalariaDocumento65 pagineTrs 398 Protocol For Photons: Moderator: Mrs. Reena Sharma Presented By: Parikshit SalariaSAlonii ChawlaNessuna valutazione finora
- Absorbed Dose Measurement Using TG-21 and TRS-398 Protocol in Electron BeamDocumento23 pagineAbsorbed Dose Measurement Using TG-21 and TRS-398 Protocol in Electron BeamSAlonii ChawlaNessuna valutazione finora
- Biodose Models:Nsd, Cre, TDF, LQ& Their Limitations: Moderator: Mr. Ranjit Singh Presented By: Navneet KaurDocumento54 pagineBiodose Models:Nsd, Cre, TDF, LQ& Their Limitations: Moderator: Mr. Ranjit Singh Presented By: Navneet KaurSAlonii ChawlaNessuna valutazione finora
- Icru-58 Recommendations For Dose Reporting: BY Pratishtha Sharma Alka Kataria Saloni ChawlaDocumento30 pagineIcru-58 Recommendations For Dose Reporting: BY Pratishtha Sharma Alka Kataria Saloni ChawlaSAlonii Chawla100% (2)
- Structure of Dicom Image in Radiology and Radiotherapy: Moderator PresenterDocumento68 pagineStructure of Dicom Image in Radiology and Radiotherapy: Moderator PresenterSAlonii ChawlaNessuna valutazione finora
- Qa&qc PDFDocumento13 pagineQa&qc PDFSAlonii ChawlaNessuna valutazione finora
- EpistaxisDocumento9 pagineEpistaxisapi-285171922Nessuna valutazione finora
- Tuberculous MeningitisDocumento34 pagineTuberculous MeningitisLuvi PujiNessuna valutazione finora
- Proposal Urogineka-DikonversiDocumento15 pagineProposal Urogineka-DikonversikamarBayi YpkmandiriNessuna valutazione finora
- 2015fenugreek PDFDocumento11 pagine2015fenugreek PDFغاز الشمالNessuna valutazione finora
- Comp. Prot. CraneoDocumento20 pagineComp. Prot. CraneoHector NuñezNessuna valutazione finora
- EPISIOTOMYDocumento17 pagineEPISIOTOMYKaye Arriane TenorioNessuna valutazione finora
- Diagnosis Management of HypertensionDocumento23 pagineDiagnosis Management of Hypertensionarahman168Nessuna valutazione finora
- Cor Triatriatum: From of Surgery and University ofDocumento9 pagineCor Triatriatum: From of Surgery and University ofAyuRizkyAndhinyNessuna valutazione finora
- Theragran (Multiple Vitamins)Documento3 pagineTheragran (Multiple Vitamins)ENessuna valutazione finora
- Banner Page: IHCP Updates Reimbursement Rate For HCPCS Code C9803, Mass Adjusts Claims That Paid IncorrectlyDocumento8 pagineBanner Page: IHCP Updates Reimbursement Rate For HCPCS Code C9803, Mass Adjusts Claims That Paid IncorrectlyIndiana Family to FamilyNessuna valutazione finora
- Therapy ModuleDocumento39 pagineTherapy ModuleSuruchi Jagdish SharmaNessuna valutazione finora
- Trauma in The Aging PopulationDocumento21 pagineTrauma in The Aging PopulationBruce Fredy Chino ChambillaNessuna valutazione finora
- 2 Prenatal CareDocumento19 pagine2 Prenatal CareShahina ShayneNessuna valutazione finora
- Nama ObatDocumento12 pagineNama Obatrolin novitaNessuna valutazione finora
- Essential - Health - Packages - Docx Filename - UTF-8''essential Health PackagesDocumento10 pagineEssential - Health - Packages - Docx Filename - UTF-8''essential Health PackagesYvonne Carmel Aguilar SunigaNessuna valutazione finora
- A. Matching Type: M: Atch The Terms in The Left Column With The Correct Descriptions in The Right ColumnDocumento9 pagineA. Matching Type: M: Atch The Terms in The Left Column With The Correct Descriptions in The Right ColumnCzarina Mae Quinones TadeoNessuna valutazione finora
- 2.manajemen Gawat Nafas Pada Bayi Dan Anak - DrlizaDocumento89 pagine2.manajemen Gawat Nafas Pada Bayi Dan Anak - DrlizayuniayuNessuna valutazione finora
- Cecilia Case Study 1 4Documento2 pagineCecilia Case Study 1 4Tugs KNessuna valutazione finora
- Wan Et Al 2019 PDFDocumento8 pagineWan Et Al 2019 PDFEdgar Huerta CardenasNessuna valutazione finora
- Side Effects of NSAIDsDocumento8 pagineSide Effects of NSAIDsAlmas PrawotoNessuna valutazione finora
- Assisting in Nasogastric Tube InsertionDocumento11 pagineAssisting in Nasogastric Tube InsertionJan Federick BantayNessuna valutazione finora
- UHS Syllabus With TOS (3rd Syllabus With TOS Year MBBS) Syllabus With TOS)Documento26 pagineUHS Syllabus With TOS (3rd Syllabus With TOS Year MBBS) Syllabus With TOS)Ali AhmadNessuna valutazione finora