Potrebbero piacerti anche
- Health Care Criteria For Performance ExcellenceDocumento2 pagineHealth Care Criteria For Performance ExcellenceLei Rivera CabulayNessuna valutazione finora
- UNIT 14 Managing Financial Resources in Health and Social CareDocumento4 pagineUNIT 14 Managing Financial Resources in Health and Social Carechandni0810Nessuna valutazione finora
- Organizational Change and DevelopmentDocumento3 pagineOrganizational Change and DevelopmentSari Marta Krisna IINessuna valutazione finora
- MIS Health Care by NaBEELDocumento10 pagineMIS Health Care by NaBEELNabeel GondalNessuna valutazione finora
- Financial Management System of Health Care OrganizationDocumento15 pagineFinancial Management System of Health Care OrganizationAmir ShahzadNessuna valutazione finora
- Role & RResponsibilities of Hospital ManagersDocumento29 pagineRole & RResponsibilities of Hospital Managersliaqat ali100% (2)
- Key Practices of Good GovernanceDocumento37 pagineKey Practices of Good GovernanceAbdisameNessuna valutazione finora
- Case ManagementDocumento7 pagineCase ManagementDev RNessuna valutazione finora
- Budgeting: Prepared By: Keizha V. RonatayDocumento19 pagineBudgeting: Prepared By: Keizha V. RonatayJericho James TopacioNessuna valutazione finora
- HRD Presentation FinalDocumento20 pagineHRD Presentation FinaldvNessuna valutazione finora
- Reflection Paper Hospital AdministrationDocumento9 pagineReflection Paper Hospital AdministrationIvy PulidoNessuna valutazione finora
- Role of Managers in HospitalsDocumento8 pagineRole of Managers in HospitalsPrathibaNessuna valutazione finora
- Hospital AdDocumento11 pagineHospital Admarketing.nexonenterprisesNessuna valutazione finora
- Four Stages of Planning and Implementation During Covid-19: One Rural Hospital'S Preparations.Documento14 pagineFour Stages of Planning and Implementation During Covid-19: One Rural Hospital'S Preparations.Irish ButtNessuna valutazione finora
- Edu Ressum Social Capital Jun2010Documento8 pagineEdu Ressum Social Capital Jun2010Swarnima TiwariNessuna valutazione finora
- Manajemen HospitalDocumento28 pagineManajemen HospitalDike Widyakti Sawfina MaharaniNessuna valutazione finora
- Internship ContentDocumento27 pagineInternship ContentmtpjusailaNessuna valutazione finora
- Hospital Management. Dr. BashaarDocumento25 pagineHospital Management. Dr. Bashaarulfat98% (49)
- Rethinking Nursing Productivity To Enhance Organizational Performance - Final - 2Documento17 pagineRethinking Nursing Productivity To Enhance Organizational Performance - Final - 2deepak162162Nessuna valutazione finora
- What Is The Role of Regulatory Agencies in Continuous Quality ImprovementDocumento14 pagineWhat Is The Role of Regulatory Agencies in Continuous Quality ImprovementJana-Tae KerrNessuna valutazione finora
- 3Documento4 pagine3Denssel TolentinoNessuna valutazione finora
- Hme 2301 Topic 1Documento8 pagineHme 2301 Topic 1Mofy AllyNessuna valutazione finora
- Public Health Care ManagementDocumento33 paginePublic Health Care Managementalexandercecilia67Nessuna valutazione finora
- Print - 1 - Foundations of High-Performing Healthcare Organizations PDFDocumento5 paginePrint - 1 - Foundations of High-Performing Healthcare Organizations PDFIntan Dwi LestariNessuna valutazione finora
- The Sullivan Hospital System ReportDocumento7 pagineThe Sullivan Hospital System ReportarvnndNessuna valutazione finora
- Organizational AnalysisDocumento7 pagineOrganizational AnalysisNursePearsonNessuna valutazione finora
- Health Systems Management 2023Documento29 pagineHealth Systems Management 2023Toto CynthiaNessuna valutazione finora
- OBM752 HM Unit-I NotesDocumento12 pagineOBM752 HM Unit-I NotesRajanNessuna valutazione finora
- Obm752 Hospital Management 1629103400 HMT NotesDocumento104 pagineObm752 Hospital Management 1629103400 HMT NotesAyisha SiddhikaNessuna valutazione finora
- Report Planning NursingServiceDocumento13 pagineReport Planning NursingServiceallanrnmanalotoNessuna valutazione finora
- Role & ResponsibilitiesDocumento24 pagineRole & ResponsibilitiesSamina JehangirNessuna valutazione finora
- CHAPTER-IV-org-ann Complete NaDocumento25 pagineCHAPTER-IV-org-ann Complete NaKyra Lalaine Angub CervantesNessuna valutazione finora
- On Hospital Financial Management (Safety & Risk Management)Documento15 pagineOn Hospital Financial Management (Safety & Risk Management)farman75% (4)
- Health Care Management PrinciplesDocumento18 pagineHealth Care Management PrinciplesFritzgerald Ace Salas PalacNessuna valutazione finora
- Auc 5Documento6 pagineAuc 5safNessuna valutazione finora
- BADVAC3X NPO Discussion - de OcampoDocumento6 pagineBADVAC3X NPO Discussion - de Ocamponaicamendoza16Nessuna valutazione finora
- Healthcare Management - PPSXDocumento16 pagineHealthcare Management - PPSXAshish SainiNessuna valutazione finora
- BudgetDocumento28 pagineBudgetRamsakal Yadav100% (1)
- Hospital Care AnsDocumento7 pagineHospital Care AnselizabethNessuna valutazione finora
- Hospital Management by Mahboob Ali KhanDocumento47 pagineHospital Management by Mahboob Ali KhanMahboob Ali KhanNessuna valutazione finora
- Cost Analysis HospitalsDocumento85 pagineCost Analysis HospitalsGeta_Varvaroi_6157100% (1)
- Liya Os Complete 2Documento61 pagineLiya Os Complete 2Twinkle VlogsNessuna valutazione finora
- Assignment 5 Public Health Preparedness 1579051Documento9 pagineAssignment 5 Public Health Preparedness 1579051Ravi KumawatNessuna valutazione finora
- Patient Relation Services Duty Manager - 130pgDocumento130 paginePatient Relation Services Duty Manager - 130pgchaithu400kvNessuna valutazione finora
- MCS in Service Organizations, Non Profit OrganizationsDocumento17 pagineMCS in Service Organizations, Non Profit OrganizationsNalini Krishnan100% (1)
- Nursing Care PlanDocumento12 pagineNursing Care PlanGladys Tamayo100% (1)
- Hospital Management: History and Introduction To HospitalDocumento22 pagineHospital Management: History and Introduction To HospitalAhmer KhanNessuna valutazione finora
- Application of Lean in Healthcare: ATANU MISRA, PRN-13020841009Documento11 pagineApplication of Lean in Healthcare: ATANU MISRA, PRN-13020841009Atanu MisraNessuna valutazione finora
- Notes - Strategic Planning in Healthcare OrganizationsDocumento7 pagineNotes - Strategic Planning in Healthcare Organizationsalodia_farichaiNessuna valutazione finora
- MCS in Service OrganisationDocumento24 pagineMCS in Service OrganisationRemy HerbieNessuna valutazione finora
- Unit 5 H SC Notes For Lesson 1 Ac1 1Documento8 pagineUnit 5 H SC Notes For Lesson 1 Ac1 1api-305415348100% (1)
- Hospital AdministrationDocumento51 pagineHospital Administrationapexcon100% (1)
- Hospital Organizational StructuresDocumento48 pagineHospital Organizational StructuresYantoNessuna valutazione finora
- 1) Essentials of Hospital Planning and AdministrationDocumento112 pagine1) Essentials of Hospital Planning and Administrationphanikr75% (16)
- Running Head: Patient-Centered Care 1Documento9 pagineRunning Head: Patient-Centered Care 1Anonymous mZC2qZNessuna valutazione finora
- Chapter 1Documento7 pagineChapter 1Jeremias Cruz CalaunanNessuna valutazione finora
- Notes on Population Health: The Healthcare GuysDa EverandNotes on Population Health: The Healthcare GuysNessuna valutazione finora
- Efficacy, Effectiveness And Efficiency In The Management Of Health SystemsDa EverandEfficacy, Effectiveness And Efficiency In The Management Of Health SystemsNessuna valutazione finora
- CE EVALUATION EXAM No. 4 - MGT, Fluid Properties, Hydrostatic Force (Answer Key)Documento6 pagineCE EVALUATION EXAM No. 4 - MGT, Fluid Properties, Hydrostatic Force (Answer Key)Angelice Alliah De la CruzNessuna valutazione finora
- Electronic Diversity Visa ProgrambDocumento1 paginaElectronic Diversity Visa Programbsamkimari5Nessuna valutazione finora
- Ethernet/Ip Parallel Redundancy Protocol: Application TechniqueDocumento50 pagineEthernet/Ip Parallel Redundancy Protocol: Application Techniquegnazareth_Nessuna valutazione finora
- 2010 - Howaldt y Schwarz - Social Innovation-Concepts, Research Fields and International - LibroDocumento82 pagine2010 - Howaldt y Schwarz - Social Innovation-Concepts, Research Fields and International - Librovallejo13Nessuna valutazione finora
- RSW - F - 01 " ": Building UtilitiesDocumento4 pagineRSW - F - 01 " ": Building Utilities62296bucoNessuna valutazione finora
- Transfert de Chaleur AngDocumento10 pagineTransfert de Chaleur Angsouhir gritliNessuna valutazione finora
- Log and Antilog TableDocumento3 pagineLog and Antilog TableDeboshri BhattacharjeeNessuna valutazione finora
- CPD - SampleDocumento3 pagineCPD - SampleLe Anh DungNessuna valutazione finora
- D E S C R I P T I O N: Acknowledgement Receipt For EquipmentDocumento2 pagineD E S C R I P T I O N: Acknowledgement Receipt For EquipmentTindusNiobetoNessuna valutazione finora
- WWW Ranker Com List Best-Isekai-Manga-Recommendations Ranker-AnimeDocumento8 pagineWWW Ranker Com List Best-Isekai-Manga-Recommendations Ranker-AnimeDestiny EasonNessuna valutazione finora
- MATM1534 Main Exam 2022 PDFDocumento7 pagineMATM1534 Main Exam 2022 PDFGiftNessuna valutazione finora
- Hyundai SL760Documento203 pagineHyundai SL760Anonymous yjK3peI7100% (3)
- PDFDocumento653 paginePDFconstantinNessuna valutazione finora
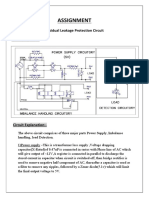
- Assignment: Residual Leakage Protection Circuit Circuit DiagramDocumento2 pagineAssignment: Residual Leakage Protection Circuit Circuit DiagramShivam ShrivastavaNessuna valutazione finora
- 11-Rubber & PlasticsDocumento48 pagine11-Rubber & PlasticsJack NgNessuna valutazione finora
- بتول ماجد سعيد (تقرير السيطرة على تلوث الهواء)Documento5 pagineبتول ماجد سعيد (تقرير السيطرة على تلوث الهواء)Batool MagedNessuna valutazione finora
- 147 Amity Avenue Nampa, ID 81937 (999) 999-9999 William at Email - ComDocumento4 pagine147 Amity Avenue Nampa, ID 81937 (999) 999-9999 William at Email - ComjeyesbelmenNessuna valutazione finora
- Diverging Lenses - Object-Image Relations: Previously in Lesson 5 Double Concave LensesDocumento2 pagineDiverging Lenses - Object-Image Relations: Previously in Lesson 5 Double Concave LensesleonNessuna valutazione finora
- Governance Operating Model: Structure Oversight Responsibilities Talent and Culture Infrastructu REDocumento6 pagineGovernance Operating Model: Structure Oversight Responsibilities Talent and Culture Infrastructu REBob SolísNessuna valutazione finora
- LC For Akij Biax Films Limited: CO2012102 0 December 22, 2020Documento2 pagineLC For Akij Biax Films Limited: CO2012102 0 December 22, 2020Mahadi Hassan ShemulNessuna valutazione finora
- JUnit 5 User GuideDocumento90 pagineJUnit 5 User GuideaawaakNessuna valutazione finora
- Daftar ObatDocumento18 pagineDaftar Obatyuyun hanakoNessuna valutazione finora
- Designed For Severe ServiceDocumento28 pagineDesigned For Severe ServiceAnthonyNessuna valutazione finora
- RH-A Catalog PDFDocumento1 paginaRH-A Catalog PDFAchmad KNessuna valutazione finora
- Atmel 46003 SE M90E32AS DatasheetDocumento84 pagineAtmel 46003 SE M90E32AS DatasheetNagarajNessuna valutazione finora
- Management Accounting by Cabrera Solution Manual 2011 PDFDocumento3 pagineManagement Accounting by Cabrera Solution Manual 2011 PDFClaudette Clemente100% (1)
- Work Energy Power SlidesDocumento36 pagineWork Energy Power Slidessweehian844100% (1)
- solidworks ขั้นพื้นฐานDocumento74 paginesolidworks ขั้นพื้นฐานChonTicha'Nessuna valutazione finora
- Functions of Theory in ResearchDocumento2 pagineFunctions of Theory in ResearchJomariMolejonNessuna valutazione finora
- Determinant of Nurses' Response Time in Emergency Department When Taking Care of A PatientDocumento9 pagineDeterminant of Nurses' Response Time in Emergency Department When Taking Care of A PatientRuly AryaNessuna valutazione finora