Potrebbero piacerti anche
- Diverticulum DiseaseDocumento6 pagineDiverticulum Diseasen_robinNessuna valutazione finora
- DiverticulosisDocumento9 pagineDiverticulosisSyafiq Shahbudin100% (1)
- UlcerativecolitisDocumento27 pagineUlcerativecolitisMohamed Abdulrazaq100% (1)
- Causes of Sis and Management of A CaseDocumento26 pagineCauses of Sis and Management of A CaseEmmanuelLazarusNessuna valutazione finora
- Diverticular Disease of The Colon: Jason Phillips, MDDocumento73 pagineDiverticular Disease of The Colon: Jason Phillips, MDfarhan adiNessuna valutazione finora
- Set 3 COMP-2Documento71 pagineSet 3 COMP-2Appu ayyalaNessuna valutazione finora
- k25 (Kelas A2) Bedah Acute AppendicitisDocumento23 paginek25 (Kelas A2) Bedah Acute Appendicitisfannie rizki anandaNessuna valutazione finora
- DIVERTIKULOSISDocumento28 pagineDIVERTIKULOSISAndrie WigunaNessuna valutazione finora
- Colon 2Documento56 pagineColon 2EnydLaRejNessuna valutazione finora
- DYSPHAGIADocumento76 pagineDYSPHAGIASaurabh AgarwalNessuna valutazione finora
- Surgery Pretest SummaryDocumento9 pagineSurgery Pretest SummaryPrince DuNessuna valutazione finora
- 5 Case Study Flood SyndromeDocumento2 pagine5 Case Study Flood SyndromeMenche DapulagNessuna valutazione finora
- Clinical Clerk Seminar Series: Approach To Gi BleedsDocumento11 pagineClinical Clerk Seminar Series: Approach To Gi BleedsAngel_Liboon_388Nessuna valutazione finora
- Appendicitis&AppendectomyDocumento5 pagineAppendicitis&AppendectomyJestine Joy CustodioNessuna valutazione finora
- Surgical Management of Ulcerative ColitisDocumento56 pagineSurgical Management of Ulcerative ColitisMehtab JameelNessuna valutazione finora
- Gallbladder DiseasesDocumento6 pagineGallbladder DiseasesJoharaNessuna valutazione finora
- Diverticulitis: Ekaterine Labadze MDDocumento11 pagineDiverticulitis: Ekaterine Labadze MDsushant jainNessuna valutazione finora
- Acute Chronic PancreatitisDocumento78 pagineAcute Chronic PancreatitisSirfaymons Sirfaymons Sirfaymons100% (1)
- Material Study Complications Gastro-Duodenal UlcersDocumento19 pagineMaterial Study Complications Gastro-Duodenal UlcersAroosha IbrahimNessuna valutazione finora
- Intestinal ObstructionDocumento15 pagineIntestinal ObstructionEmmeline Dycangchon-GarmaNessuna valutazione finora
- Diverticular Disease of The ColonDocumento38 pagineDiverticular Disease of The Colonapi-19641337Nessuna valutazione finora
- 2 Gastric and Duodenal Peptic Ulcer Disease 2Documento35 pagine2 Gastric and Duodenal Peptic Ulcer Disease 2rayNessuna valutazione finora
- Dayrit, Zandra Chris S.: What Is Pancreatitis?Documento5 pagineDayrit, Zandra Chris S.: What Is Pancreatitis?Nicole Anne TungolNessuna valutazione finora
- Whipple's OperationDocumento35 pagineWhipple's OperationSunaina AdhikariNessuna valutazione finora
- Diverticular Disease: Diverticulitis, Bleeding, and FistulaDocumento8 pagineDiverticular Disease: Diverticulitis, Bleeding, and FistulaakashkumarpanwarNessuna valutazione finora
- Peptic Ulcer Disease: by Parthevan RajasingamDocumento33 paginePeptic Ulcer Disease: by Parthevan RajasingamNinaNessuna valutazione finora
- Inflammatory Bowel Disease (Ibd)Documento28 pagineInflammatory Bowel Disease (Ibd)suhaNessuna valutazione finora
- There Are Many Potential Causes of Liver AbscessesDocumento4 pagineThere Are Many Potential Causes of Liver AbscessesmarianmadhurNessuna valutazione finora
- Small Intestine and ColonDocumento9 pagineSmall Intestine and Colonlentini@maltanet.netNessuna valutazione finora
- Inflammatoray Bowel DiseaseDocumento14 pagineInflammatoray Bowel DiseaseSadr AkrmNessuna valutazione finora
- Pancreatitis Ercp Pain Amylase Lipase ErcpDocumento24 paginePancreatitis Ercp Pain Amylase Lipase ErcpPerplexed CeleryNessuna valutazione finora
- CHOLEDocumento25 pagineCHOLEJane TuazonNessuna valutazione finora
- Basic Knowledge GitDocumento20 pagineBasic Knowledge GitFajar Dan SenjaNessuna valutazione finora
- General Pathology Single Best Answers For The MRCSDocumento22 pagineGeneral Pathology Single Best Answers For The MRCStahir_the_great2939Nessuna valutazione finora
- The Acute Abdomen: Chapter OutlineDocumento19 pagineThe Acute Abdomen: Chapter OutlineGabriella TjondroNessuna valutazione finora
- Surgery Class Biliary System SurgeryDocumento69 pagineSurgery Class Biliary System SurgeryKashif BurkiNessuna valutazione finora
- Peptic Ulcer Disease: Palangka Raya University Faculty of MedicineDocumento70 paginePeptic Ulcer Disease: Palangka Raya University Faculty of MedicineMITHA100% (1)
- Diverticular Disease Diagnosis and TreatmentDocumento6 pagineDiverticular Disease Diagnosis and TreatmentKhasandra PacioNessuna valutazione finora
- Abdominal X-Rays PT 1Documento20 pagineAbdominal X-Rays PT 1sb medexNessuna valutazione finora
- What Is An Acute AbdomenDocumento112 pagineWhat Is An Acute AbdomenLavasa SharmaNessuna valutazione finora
- Gastrointestinal System Block: Case 5ADocumento12 pagineGastrointestinal System Block: Case 5ARonald ChrisbiantoNessuna valutazione finora
- Small & Large Intestines - LectureDocumento70 pagineSmall & Large Intestines - Lecturehussain AltaherNessuna valutazione finora
- K-25 Acute AppendicitisDocumento23 pagineK-25 Acute AppendicitiscarinasheliapNessuna valutazione finora
- Diverticulitis Cure: The Ultimate Diverticulitis Diet: Diverticulitis Recipes: Your Ultimate Diverticulitis CookbookDa EverandDiverticulitis Cure: The Ultimate Diverticulitis Diet: Diverticulitis Recipes: Your Ultimate Diverticulitis CookbookNessuna valutazione finora
- Complications of PancratitisDocumento14 pagineComplications of PancratitisjulieNessuna valutazione finora
- Approach Considerations: Ercutaneous DrainageDocumento35 pagineApproach Considerations: Ercutaneous DrainageWorku KifleNessuna valutazione finora
- Acute Cholecystitis:: Etiological TypesDocumento5 pagineAcute Cholecystitis:: Etiological Typesvivek yadavNessuna valutazione finora
- Mrcs Upper GitDocumento59 pagineMrcs Upper GitAdebisiNessuna valutazione finora
- Acute Pancreatitis: Presenter:Luqman Arif Bin Ahmad Hazri Supervisor: DR DarrenDocumento25 pagineAcute Pancreatitis: Presenter:Luqman Arif Bin Ahmad Hazri Supervisor: DR DarrenLuqman Arif Ahmad HazriNessuna valutazione finora
- CholecystitisDocumento12 pagineCholecystitisMariela HuertaNessuna valutazione finora
- Vascular Disease of The BowelDocumento28 pagineVascular Disease of The BowelOlga GoryachevaNessuna valutazione finora
- DiverticulitisDocumento23 pagineDiverticulitisSuhanda SaputraNessuna valutazione finora
- Colonic and Small Intestine Disorders-1Documento28 pagineColonic and Small Intestine Disorders-1YIKI ISAACNessuna valutazione finora
- Colelitiasis SD MirizziDocumento14 pagineColelitiasis SD MirizziPipex Del MorroNessuna valutazione finora
- Upper Gastrointestinal BleedingDocumento46 pagineUpper Gastrointestinal BleedingRashed ShatnawiNessuna valutazione finora
- Biliary Diseases: Dr. Wu Yang Dept. of Surgery The First Affiliated Hospital of Zhengzhou UniversityDocumento42 pagineBiliary Diseases: Dr. Wu Yang Dept. of Surgery The First Affiliated Hospital of Zhengzhou Universityapi-19916399Nessuna valutazione finora
- Cholecystitis FinalDocumento57 pagineCholecystitis FinalRajendra DesaiNessuna valutazione finora
- No Gallbladder Diet Cookbook: Discover Flavorful and Nourishing Recipes to Revitalize Your Metabolism After Gallbladder Surgery [III EDITION]Da EverandNo Gallbladder Diet Cookbook: Discover Flavorful and Nourishing Recipes to Revitalize Your Metabolism After Gallbladder Surgery [III EDITION]Valutazione: 5 su 5 stelle5/5 (24)
- Catheters and Guide Wires: Presenter: Omkar Gaonkar Course: M.SC., Mit 2 SEM Moderator: Kayalvizhi R DATE:26/03/2019Documento42 pagineCatheters and Guide Wires: Presenter: Omkar Gaonkar Course: M.SC., Mit 2 SEM Moderator: Kayalvizhi R DATE:26/03/2019Omkar GaonkarNessuna valutazione finora
- Budget Plan Wound ClinicDocumento4 pagineBudget Plan Wound ClinicRegalado Aguhayon100% (1)
- Use of Oral Sucrose 08Documento16 pagineUse of Oral Sucrose 08madimadi11Nessuna valutazione finora
- Abdomen CAP Questions and AnswersDocumento6 pagineAbdomen CAP Questions and AnswersRathnaNessuna valutazione finora
- Brazil Normative Instruction in No 2 31may2011 enDocumento3 pagineBrazil Normative Instruction in No 2 31may2011 enLackner MarceloNessuna valutazione finora
- Surgical InstrumentsDocumento49 pagineSurgical Instrumentsjisoo100% (1)
- Shahzad G. Raja - Cardiac Surgery - A Complete Guide-Springer (2020)Documento1.043 pagineShahzad G. Raja - Cardiac Surgery - A Complete Guide-Springer (2020)sebaedmund1999Nessuna valutazione finora
- Red Flag Symptoms - Abdominal Pain - GPonlineDocumento7 pagineRed Flag Symptoms - Abdominal Pain - GPonlinedrsadafrafiNessuna valutazione finora
- Mod9Week3 - PA 3306 - Sept 5&6Documento22 pagineMod9Week3 - PA 3306 - Sept 5&6komal sheikhNessuna valutazione finora
- FGU Skill SheetDocumento1 paginaFGU Skill SheetMuhammed ElgasimNessuna valutazione finora
- Indravati PCPNDT 2 MoDocumento6 pagineIndravati PCPNDT 2 MoDr Sachin Chitnis M O UPHC AiroliNessuna valutazione finora
- Movements at The Hip and Muscles-O, I, NSDocumento7 pagineMovements at The Hip and Muscles-O, I, NSKrissy WilhelmsenNessuna valutazione finora
- Kelompok 4 - 1B - Temporomandibular JointDocumento25 pagineKelompok 4 - 1B - Temporomandibular JointLutfi HanifahNessuna valutazione finora
- G Epl PDFDocumento39 pagineG Epl PDFSaenab AminNessuna valutazione finora
- Inguinal HerniaDocumento4 pagineInguinal HerniaRegine SitchonNessuna valutazione finora
- BIRADSDocumento94 pagineBIRADSSergio MoralesNessuna valutazione finora
- 3D Mapping Expert Consensus JoADocumento34 pagine3D Mapping Expert Consensus JoAFikriYTNessuna valutazione finora
- Choque HemorragicoDocumento9 pagineChoque HemorragicoAna NevesNessuna valutazione finora
- Nejm How To PericardiocentesisDocumento5 pagineNejm How To Pericardiocentesispkapur8552Nessuna valutazione finora
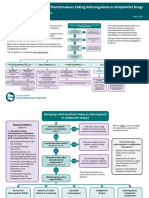
- Sdcep Anticoagulants Quick Reference Guide 2nd EditionDocumento5 pagineSdcep Anticoagulants Quick Reference Guide 2nd EditionMeryem LahlouNessuna valutazione finora
- Wilmes. and Ludwig - Mini-Implants in The Anterior PalateDocumento64 pagineWilmes. and Ludwig - Mini-Implants in The Anterior Palateromulodent100% (1)
- NCMB316: Compilation Finals in NCMB316Documento23 pagineNCMB316: Compilation Finals in NCMB316Armand Bong Santiago100% (1)
- RLE Procedure NCM 109Documento59 pagineRLE Procedure NCM 109robertvaliente471Nessuna valutazione finora
- Uworld Step 2 CK Charts-OcrDocumento440 pagineUworld Step 2 CK Charts-OcrIvory Jameston100% (2)
- Radiology Report 2300985Documento4 pagineRadiology Report 2300985JyotiNessuna valutazione finora
- RADIOLOGY MultipleQuestionsDocumento6 pagineRADIOLOGY MultipleQuestionsخلدون سليم100% (1)
- Cosmetic Derm PDFDocumento1.170 pagineCosmetic Derm PDFhesham100% (3)
- A Simple Technique To Measure The Volume of Removed Buccal FatDocumento3 pagineA Simple Technique To Measure The Volume of Removed Buccal FatGuilherme GuerraNessuna valutazione finora
- Ileo Biliar Inukai 2019Documento4 pagineIleo Biliar Inukai 2019stefanyNessuna valutazione finora
- List For 3 Cases & 1 Emergency Case: Description of Consumables QTYDocumento2 pagineList For 3 Cases & 1 Emergency Case: Description of Consumables QTYmirabelle LovethNessuna valutazione finora

























































![No Gallbladder Diet Cookbook: Discover Flavorful and Nourishing Recipes to Revitalize Your Metabolism After Gallbladder Surgery [III EDITION]](https://imgv2-1-f.scribdassets.com/img/word_document/591540228/149x198/6ba6cc3b38/1713999276?v=1)