Potrebbero piacerti anche
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- Neutropenic SepsisDocumento38 pagineNeutropenic SepsisYS NateNessuna valutazione finora
- Filaria PPT - ClassDocumento59 pagineFilaria PPT - ClassGauravMeratwal100% (2)
- Introduction To MicrobiologyDocumento55 pagineIntroduction To Microbiologymeldestacamentojr100% (3)
- Scabies and PediculosisDocumento35 pagineScabies and PediculosisleenaloveuNessuna valutazione finora
- IMO Soal MCQDocumento4 pagineIMO Soal MCQWenny MonicaNessuna valutazione finora
- Immunology and Serology NotesDocumento171 pagineImmunology and Serology NotesMa Loidette Rull Guanlao-Serrano67% (3)
- Class XI Biology Support MaterialDocumento248 pagineClass XI Biology Support MaterialPranav Pratap Singh100% (1)
- Commonly Used ICD-10 Procedure CodesDocumento1 paginaCommonly Used ICD-10 Procedure CodesMonika Putong PaatNessuna valutazione finora
- Local Anesthetics and Regional TechniquesDocumento41 pagineLocal Anesthetics and Regional TechniquesMuhamad Agung SupriyantoNessuna valutazione finora
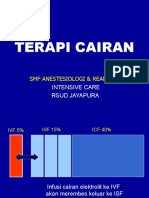
- Terapi CairanDocumento31 pagineTerapi CairanInggriht Senny BondangNessuna valutazione finora
- JURNAL in EnglishDocumento24 pagineJURNAL in EnglishMonika Putong PaatNessuna valutazione finora
- Jadwal Jaga Malam IGDDocumento1 paginaJadwal Jaga Malam IGDMonika Putong PaatNessuna valutazione finora
- Socket An OftalmicDocumento15 pagineSocket An OftalmicMonika Putong PaatNessuna valutazione finora
- WPW and AV Block ChaptersDocumento33 pagineWPW and AV Block ChaptersMonika Putong PaatNessuna valutazione finora
- Socket An OftalmicDocumento15 pagineSocket An OftalmicMonika Putong PaatNessuna valutazione finora
- Link Journal KedokteranDocumento2 pagineLink Journal KedokteranMonika Putong PaatNessuna valutazione finora
- Coass Jaga: Arfadin, Anastasia, Benny, Cykita, Ratna, Galuh, Yolanda, OctoviantiDocumento11 pagineCoass Jaga: Arfadin, Anastasia, Benny, Cykita, Ratna, Galuh, Yolanda, OctoviantiMonika Putong PaatNessuna valutazione finora
- Morning Report 28 Juni 2017Documento11 pagineMorning Report 28 Juni 2017Monika Putong PaatNessuna valutazione finora
- Knowledge, Attitudes and Practices on Dengue Fever among Slum DwellersDocumento11 pagineKnowledge, Attitudes and Practices on Dengue Fever among Slum DwellersMahadie Hasan JahadNessuna valutazione finora
- Acute Otitis Media: Dr. Ajay Manickam Junior Resident RG Kar Medical College HospitalDocumento20 pagineAcute Otitis Media: Dr. Ajay Manickam Junior Resident RG Kar Medical College HospitalchawkatNessuna valutazione finora
- Wrights 1 StepDocumento7 pagineWrights 1 StepJoyce YapNessuna valutazione finora
- Herpes ZosterDocumento12 pagineHerpes ZosterCharlz ZipaganNessuna valutazione finora
- QUESTIONS AND ANSWERS: CARDIOLOGY AND NEUROLOGYDocumento117 pagineQUESTIONS AND ANSWERS: CARDIOLOGY AND NEUROLOGYMenna GalalNessuna valutazione finora
- CH. 26 Microbial Diseases of The Urinary and Reproductive SystemsDocumento3 pagineCH. 26 Microbial Diseases of The Urinary and Reproductive SystemstkanesNessuna valutazione finora
- Pityrosporum FolliculitisDocumento3 paginePityrosporum Folliculitisshivam18Nessuna valutazione finora
- Fever and Rash in The Immunocompetent PatientDocumento62 pagineFever and Rash in The Immunocompetent PatientsunilchhajwaniNessuna valutazione finora
- Enhanced Rice Resistance to Fungal Disease via SA Pathway and WRKY45Documento4 pagineEnhanced Rice Resistance to Fungal Disease via SA Pathway and WRKY45Glen TrinidadNessuna valutazione finora
- Bacterial Artificial ChromosomeDocumento3 pagineBacterial Artificial ChromosomeNTA UGC-NETNessuna valutazione finora
- Profil Pasien Tuberkulosis Berat Dalam Perawatan Inap Di Rumah Sakit Cipto Mangunkusumo, JakartaDocumento5 pagineProfil Pasien Tuberkulosis Berat Dalam Perawatan Inap Di Rumah Sakit Cipto Mangunkusumo, JakartaDian Putri NingsihNessuna valutazione finora
- Pharmaceutics 13 01077Documento24 paginePharmaceutics 13 01077Rasha ElbannaNessuna valutazione finora
- Royal Pain: Egypt at A GlanceDocumento3 pagineRoyal Pain: Egypt at A GlanceRajendra PilludaNessuna valutazione finora
- The Final - Assignment Typhoid MaryDocumento4 pagineThe Final - Assignment Typhoid Maryapi-311342690Nessuna valutazione finora
- Coccidia: - Characterized by Thick-Walled OocystsDocumento26 pagineCoccidia: - Characterized by Thick-Walled Oocyststaty jatyNessuna valutazione finora
- Microbiology and Parasitology 100: Trinity University of Asia St. Luke's College of NursingDocumento11 pagineMicrobiology and Parasitology 100: Trinity University of Asia St. Luke's College of NursingFereli Joy SupanNessuna valutazione finora
- AMI Equipment Services and Solutions, Inc. Biomedical Engineering DepartmentDocumento11 pagineAMI Equipment Services and Solutions, Inc. Biomedical Engineering Departmentvandolph siribanNessuna valutazione finora
- Bacteremia Fungemia, and Blood Cul Tures-V1Documento53 pagineBacteremia Fungemia, and Blood Cul Tures-V1Alok MishraNessuna valutazione finora
- B.SC MicroBiology Syllubus 01.01.2017Documento42 pagineB.SC MicroBiology Syllubus 01.01.2017VenkataMurali KrishnaNessuna valutazione finora
- Memorias XL Congreso Nacional Microbiologia 1Documento323 pagineMemorias XL Congreso Nacional Microbiologia 1XsiSkullNessuna valutazione finora
- Specific Immune System: T - LymphocytesDocumento18 pagineSpecific Immune System: T - Lymphocytesarun231187Nessuna valutazione finora
- Know About Dengue FeverDocumento11 pagineKnow About Dengue FeverKamlesh SanghaviNessuna valutazione finora
- Tarif 2018 Rev 9 Wil 3-New (Kirim Kontraktor)Documento27 pagineTarif 2018 Rev 9 Wil 3-New (Kirim Kontraktor)Aprillia PutrieNessuna valutazione finora