Potrebbero piacerti anche
- TBC Paru Pada Anak: Blok Respiro (K24, K25)Documento59 pagineTBC Paru Pada Anak: Blok Respiro (K24, K25)Fkumi 2019Nessuna valutazione finora
- PneumoniaDocumento105 paginePneumoniaPrateek Kumar PandaNessuna valutazione finora
- Journal Homepage: - : IntroductionDocumento5 pagineJournal Homepage: - : IntroductionIJAR JOURNALNessuna valutazione finora
- TB PedDocumento34 pagineTB PedSebastián NovoaNessuna valutazione finora
- 6 COMMUNICABLE DISEASES Nies PDocumento14 pagine6 COMMUNICABLE DISEASES Nies PMontero, Ma. Cecilia - BSN 3-BNessuna valutazione finora
- Deep Fungal InfectionDocumento39 pagineDeep Fungal InfectionFahmi Nur AL-HidayatNessuna valutazione finora
- Pediatric TuberculosisDocumento126 paginePediatric TuberculosisSherly CanceritaNessuna valutazione finora
- Vaccine Preventable DiseasesDocumento62 pagineVaccine Preventable DiseasesAngela Joy AmparadoNessuna valutazione finora
- Dr. R V S N Sarma., MD., MSC., (Canada) Consultant Physician & Chest Specialist Visit Us At: WWW - Drsarma.InDocumento76 pagineDr. R V S N Sarma., MD., MSC., (Canada) Consultant Physician & Chest Specialist Visit Us At: WWW - Drsarma.InAndry Wahyudi AgusNessuna valutazione finora
- Pediatric TB Management Training Diagnosis (Part 2Documento56 paginePediatric TB Management Training Diagnosis (Part 2Irfandy Chairi Sulaiman LubisNessuna valutazione finora
- Diagnosis TBDocumento44 pagineDiagnosis TBGede Eka Putra NugrahaNessuna valutazione finora
- Current Management of Fungal Urinary Tract Infection and FunguriaDocumento47 pagineCurrent Management of Fungal Urinary Tract Infection and FunguriaFeysel JemalNessuna valutazione finora
- New Diagnostic Approach of Pneumonia - Prof AryatiDocumento52 pagineNew Diagnostic Approach of Pneumonia - Prof AryatiyanuarizkaNessuna valutazione finora
- Articulos de Divulgacion2016Documento1 paginaArticulos de Divulgacion2016Ivan Mauricio TrompaNessuna valutazione finora
- Covid 19 Guidelines April 2021Documento42 pagineCovid 19 Guidelines April 2021K.sushmaNessuna valutazione finora
- San Laz High Yield ReviewerDocumento5 pagineSan Laz High Yield ReviewerKen Edward ZataNessuna valutazione finora
- Delayed Cancer Diagnoses and High Mortality in Children During The COVID 19 PandemicDocumento3 pagineDelayed Cancer Diagnoses and High Mortality in Children During The COVID 19 PandemicJohannaNessuna valutazione finora
- Chlamydia Infection Causes and SymptomsDocumento45 pagineChlamydia Infection Causes and Symptomsmnn164Nessuna valutazione finora
- Laboratory Report: Name: MR .Sandeep Mane Patient ID: P80359Documento1 paginaLaboratory Report: Name: MR .Sandeep Mane Patient ID: P80359akash srivastavaNessuna valutazione finora
- The Basic concept of Prudent Use of antimicrobial drugDocumento40 pagineThe Basic concept of Prudent Use of antimicrobial drugBerkatnu Indrawan JangukNessuna valutazione finora
- DR Sudhir Bhandari Final Presentation 12-4-2021 NewDocumento67 pagineDR Sudhir Bhandari Final Presentation 12-4-2021 NewsurruNessuna valutazione finora
- Nursing Care of The Community: Control of Communicable Diseases Instructional SlidesDocumento46 pagineNursing Care of The Community: Control of Communicable Diseases Instructional SlidesJullienne Ysabelle AngNessuna valutazione finora
- CNS Toxoplasmosis in Syndrome: Clinical-Pathological-Radiological ofDocumento6 pagineCNS Toxoplasmosis in Syndrome: Clinical-Pathological-Radiological ofKevinJuliusTanadyNessuna valutazione finora
- Blueprint Ukai Osce 2017Documento66 pagineBlueprint Ukai Osce 2017Uci RamadhaniNessuna valutazione finora
- Clinical and Histopathological Correlation of Cutaneous TuberculosisDocumento6 pagineClinical and Histopathological Correlation of Cutaneous Tuberculosisderil ridwanNessuna valutazione finora
- Iuatld Chesttb Atlas Kids PDFDocumento65 pagineIuatld Chesttb Atlas Kids PDFtomeyttoNessuna valutazione finora
- Tuberkulosis Anak: Dr. Dewi Angreany M.Ked (Ped), Sp.ADocumento52 pagineTuberkulosis Anak: Dr. Dewi Angreany M.Ked (Ped), Sp.AIlham KurniawanNessuna valutazione finora
- Spectrum of Clinicopathologic Findings in COVID-19-induced Skin LesionsDocumento9 pagineSpectrum of Clinicopathologic Findings in COVID-19-induced Skin LesionsggenesisNessuna valutazione finora
- DR - PARTHA - 2018 Clinical Microbiology II PDFDocumento88 pagineDR - PARTHA - 2018 Clinical Microbiology II PDFNuzki YofandaNessuna valutazione finora
- Jurnal Candida 1Documento4 pagineJurnal Candida 1ismirandaNessuna valutazione finora
- Tandoc A,+12 PJP Vol7+no2 07-02-BC-01 4ppDocumento4 pagineTandoc A,+12 PJP Vol7+no2 07-02-BC-01 4pprachelNessuna valutazione finora
- Spleniic TBDocumento6 pagineSpleniic TBDwi Ayu LestariNessuna valutazione finora
- E005427 FullDocumento12 pagineE005427 FullTarandam INessuna valutazione finora
- DR Irawaty CAP MANAGEMENT UPDATE BASED ON NEW GUIDELINESDocumento35 pagineDR Irawaty CAP MANAGEMENT UPDATE BASED ON NEW GUIDELINESKornelis AribowoNessuna valutazione finora
- Pediatric Department Faculty of MedicineDocumento100 paginePediatric Department Faculty of MedicineIrfanNessuna valutazione finora
- Pulmonary Endemic MycosesDocumento4 paginePulmonary Endemic MycosesFamilia CarbajalNessuna valutazione finora
- Critical Care Beyond The Picu, Since The Emergency Room: How Come The Pediatric Intensivist Be A Covidologist?Documento44 pagineCritical Care Beyond The Picu, Since The Emergency Room: How Come The Pediatric Intensivist Be A Covidologist?adeNessuna valutazione finora
- Oamjms 10b 1869Documento7 pagineOamjms 10b 1869christina kusuma reniNessuna valutazione finora
- Yun AidaDocumento7 pagineYun AidaAisyah ElmarussyNessuna valutazione finora
- Healthcare Associated Infections in The Nicu PowerpointDocumento21 pagineHealthcare Associated Infections in The Nicu Powerpointapi-489132887Nessuna valutazione finora
- Computed Tomographic Features of Pulmonary Mucormycosis Among Covid 19 Survivors A Diagnostic ChallengeDocumento9 pagineComputed Tomographic Features of Pulmonary Mucormycosis Among Covid 19 Survivors A Diagnostic ChallengeInternational Journal of Innovative Science and Research TechnologyNessuna valutazione finora
- How Do I Manage Nocardiosis?Documento9 pagineHow Do I Manage Nocardiosis?Dan JaiNessuna valutazione finora
- DHIS Monthly Reporting Form PHC FacilitiesDocumento4 pagineDHIS Monthly Reporting Form PHC FacilitiesVampire OnFireNessuna valutazione finora
- 2022 Article 13495Documento12 pagine2022 Article 13495vuongquynh290900Nessuna valutazione finora
- Seminario 6 Inmunologia Clinica 2023-IIDocumento15 pagineSeminario 6 Inmunologia Clinica 2023-IImiguel angel ascoy saucedoNessuna valutazione finora
- Scrofuloderma: Images in DermatologyDocumento1 paginaScrofuloderma: Images in DermatologyAkira MasumiNessuna valutazione finora
- Mediastinal Granulomatous Lymphadenitis in A Population at Risk For HIV and TuberculosisDocumento6 pagineMediastinal Granulomatous Lymphadenitis in A Population at Risk For HIV and TuberculosisJorge Manuel Tantachuco RuizNessuna valutazione finora
- Candidiasis in PICUDocumento6 pagineCandidiasis in PICUMeirinda HidayantiNessuna valutazione finora
- Disease of Endocardium, Myocardium and PericardiumDocumento54 pagineDisease of Endocardium, Myocardium and PericardiumadystiNessuna valutazione finora
- Neonates Hospitalized With Community-Acquired Sars-Cov-2 in A Colorado Neonatal Intensive Care UnitDocumento5 pagineNeonates Hospitalized With Community-Acquired Sars-Cov-2 in A Colorado Neonatal Intensive Care UnitRosario DonosoNessuna valutazione finora
- Pneumonia: Dr. Tjatur Winarsanto SPPDDocumento46 paginePneumonia: Dr. Tjatur Winarsanto SPPDanisamayaNessuna valutazione finora
- SyphilisDocumento24 pagineSyphilisEvaG2012Nessuna valutazione finora
- TB Paru FK UncenDocumento66 pagineTB Paru FK UncenAndira Trianingrum TukanNessuna valutazione finora
- PNEUMONIA: Phases, Manifestations, and DiagnosisDocumento47 paginePNEUMONIA: Phases, Manifestations, and DiagnosisNica Lopez FernandezNessuna valutazione finora
- DR As TuberculosisDocumento59 pagineDR As TuberculosisAchhar SinghNessuna valutazione finora
- Management of Mild Cases of COVID-19 in Low-Resource CountriesDocumento2 pagineManagement of Mild Cases of COVID-19 in Low-Resource CountriesAnthony HopkinsNessuna valutazione finora
- Antibiotics 11 01804 v2Documento15 pagineAntibiotics 11 01804 v2pedro villegasNessuna valutazione finora
- Diagnosis of CandediasisDocumento15 pagineDiagnosis of Candediasismahbub alamNessuna valutazione finora
- You Are Infected and You Don't Even Know It: The Viruses, Bacteria, and Parasites Already Inside YouDa EverandYou Are Infected and You Don't Even Know It: The Viruses, Bacteria, and Parasites Already Inside YouValutazione: 5 su 5 stelle5/5 (1)
- Infections in Cancer Chemotherapy: A Symposium Held at the Institute Jules Bordet, Brussels, BelgiumDa EverandInfections in Cancer Chemotherapy: A Symposium Held at the Institute Jules Bordet, Brussels, BelgiumNessuna valutazione finora
- Practical Pediatric TB Scoring System for DiagnosisDocumento5 paginePractical Pediatric TB Scoring System for DiagnosisM Rizky Assilmy LubisNessuna valutazione finora
- Hypoplasia of The Lung: Helmilubis Ridwanm. Daulay Wismandalimunthe RinisavitridaulayDocumento29 pagineHypoplasia of The Lung: Helmilubis Ridwanm. Daulay Wismandalimunthe RinisavitridaulayM Rizky Assilmy LubisNessuna valutazione finora
- What? Who?: DR - Mabel Sihombing Sppd-Kgeh DR - Ilhamd SPPD Dpertemen Ilmu Penyakit Dalam Rs - Ham/Fk-Usu MedanDocumento45 pagineWhat? Who?: DR - Mabel Sihombing Sppd-Kgeh DR - Ilhamd SPPD Dpertemen Ilmu Penyakit Dalam Rs - Ham/Fk-Usu MedanM Rizky Assilmy LubisNessuna valutazione finora
- A6. Tukak PeptikDocumento31 pagineA6. Tukak PeptikSartika NapitupuluNessuna valutazione finora
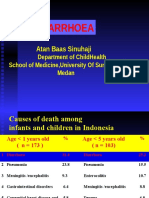
- Diarrhoea: Atan Baas SinuhajiDocumento45 pagineDiarrhoea: Atan Baas SinuhajiMeirani RizdaputriNessuna valutazione finora
- (K12) Penataan Besi ParenteralDocumento15 pagine(K12) Penataan Besi ParenteralM Rizky Assilmy LubisNessuna valutazione finora
- (SDH) K11 - AnemiaDocumento17 pagine(SDH) K11 - AnemiaHanda YaniNessuna valutazione finora
- Aitc 2021Documento2 pagineAitc 2021Jetbar Dolok SaribuNessuna valutazione finora
- Rajiv Gandhi University of Health Sciences Exam Result: PrintDocumento1 paginaRajiv Gandhi University of Health Sciences Exam Result: PrintDani ursNessuna valutazione finora
- Arellano University: Andres Bonifacio Campus College of Arts and Sciences Psychology DepartmentDocumento97 pagineArellano University: Andres Bonifacio Campus College of Arts and Sciences Psychology DepartmentJohn Michael MortidoNessuna valutazione finora
- NEBOSH IGC1 Past Exam Paper March 2012Documento3 pagineNEBOSH IGC1 Past Exam Paper March 2012Seleni100% (1)
- Nursing Student Cover LetterDocumento8 pagineNursing Student Cover Letterafmrpaxgfqdkor100% (1)
- User Manual 2 3875358Documento23 pagineUser Manual 2 3875358Maria Camila RestrepoNessuna valutazione finora
- The Battle Against Workplace Stress - PDF Read ArticleDocumento12 pagineThe Battle Against Workplace Stress - PDF Read ArticleRama KrishnaNessuna valutazione finora
- Home Remedies For UtiDocumento5 pagineHome Remedies For UtiShiro KiryuuNessuna valutazione finora
- Perioperative Care of The Child: A Nursing Manual: October 2010 Vol 92 No4Documento2 paginePerioperative Care of The Child: A Nursing Manual: October 2010 Vol 92 No4Pahang Reforansa PutraNessuna valutazione finora
- Pediculosis: Pubis (Pubic Louse)Documento4 paginePediculosis: Pubis (Pubic Louse)christian quiaoitNessuna valutazione finora
- Levothyroxine (Synthroid)Documento1 paginaLevothyroxine (Synthroid)E50% (2)
- Quickstart Guide To Microdosing Magic Mushrooms v1Documento17 pagineQuickstart Guide To Microdosing Magic Mushrooms v1plasmalasgun100% (2)
- Effects of Implementation of Focus-Pdca Model OnDocumento14 pagineEffects of Implementation of Focus-Pdca Model OnSofiyullohNessuna valutazione finora
- EAC School of Nursing Case Analysis on Hyperemesis GravidarumDocumento8 pagineEAC School of Nursing Case Analysis on Hyperemesis GravidarumcchiechieNessuna valutazione finora
- Adolescent Romantic Relationships (Article) Author Sarah SorensenDocumento4 pagineAdolescent Romantic Relationships (Article) Author Sarah SorensenDavidNessuna valutazione finora
- An Auricular Marker For Covid-19: Nadia Volf, MD, PHD, Valery Salques, MD, and Anne Lassaux, MDDocumento2 pagineAn Auricular Marker For Covid-19: Nadia Volf, MD, PHD, Valery Salques, MD, and Anne Lassaux, MDyan92120Nessuna valutazione finora
- Ethico-Legal Considerations in Conducting Health EducationDocumento45 pagineEthico-Legal Considerations in Conducting Health EducationSherwyn Uy Hatab100% (1)
- The United States Health Care System Combining Business Health and Delivery 2nd Edition Austin Wetle Test BankDocumento10 pagineThe United States Health Care System Combining Business Health and Delivery 2nd Edition Austin Wetle Test BankMichaelBlairozrc100% (27)
- First Aid: NSTP 002Documento5 pagineFirst Aid: NSTP 002Alvin VelasquezNessuna valutazione finora
- BSBHRM506 Assessment 1Documento9 pagineBSBHRM506 Assessment 1prasannareddy9989Nessuna valutazione finora
- Anti TB PPT FinalDocumento43 pagineAnti TB PPT FinalKeziah GillNessuna valutazione finora
- Alterations With Infectious, Inflammatory and Immunologic ResponsesDocumento8 pagineAlterations With Infectious, Inflammatory and Immunologic ResponsesPATRIZJA YSABEL REYESNessuna valutazione finora
- Lesson PlanDocumento7 pagineLesson PlanMr. khanNessuna valutazione finora
- Agaricus Muscaria FungusDocumento2 pagineAgaricus Muscaria FungusRemus BabeuNessuna valutazione finora
- Psychiatric Nursing Download ReviewerDocumento9 paginePsychiatric Nursing Download Reviewerkarenkaren09Nessuna valutazione finora
- خارطة اختبار الترميز الطبيDocumento3 pagineخارطة اختبار الترميز الطبيANFALNessuna valutazione finora
- Eastern Connecticut State University Informed Consent Form: Participant's Printed NameDocumento4 pagineEastern Connecticut State University Informed Consent Form: Participant's Printed NameKisu Hive GamesNessuna valutazione finora
- Concept of Stress and Psychological Adaptation To StressDocumento12 pagineConcept of Stress and Psychological Adaptation To Stressvaideeswari kumarNessuna valutazione finora
- Tsca Toxic Substanteces Control ActDocumento1 paginaTsca Toxic Substanteces Control ActAlbert Casanova FernandezNessuna valutazione finora
- PAR-Q General Health ScreeningDocumento2 paginePAR-Q General Health ScreeningJello UcagNessuna valutazione finora