Potrebbero piacerti anche
- A Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsDa EverandA Simple Guide to Hypovolemia, Diagnosis, Treatment and Related ConditionsNessuna valutazione finora
- Arterial Line Arterial LineDocumento13 pagineArterial Line Arterial LineLinamaria Lozano100% (1)
- Respiratory Assessment 2Documento24 pagineRespiratory Assessment 2Kendal BartonNessuna valutazione finora
- Case Presentation: DR - Anbalagan II ND Year MEMDocumento20 pagineCase Presentation: DR - Anbalagan II ND Year MEMDr mahi sNessuna valutazione finora
- Abdominal Swelling + AscitesDocumento29 pagineAbdominal Swelling + AscitesDevina CiayadiNessuna valutazione finora
- Right Sided Heart FailureDocumento33 pagineRight Sided Heart FailurePaulNessuna valutazione finora
- ENT Nursing Care GuideDocumento32 pagineENT Nursing Care GuideabdulNessuna valutazione finora
- Cardiovascular System Diseases Part 2Documento9 pagineCardiovascular System Diseases Part 2Prince Rener Velasco PeraNessuna valutazione finora
- CARDIOVASCULAR DISEASES: SIGNS, SYMPTOMS AND TREATMENT OF HEART FAILUREDocumento27 pagineCARDIOVASCULAR DISEASES: SIGNS, SYMPTOMS AND TREATMENT OF HEART FAILURESanthoshi Sadhanaa SankarNessuna valutazione finora
- IV Fluid ChartDocumento2 pagineIV Fluid Charthady920Nessuna valutazione finora
- Chronic Obstructive Pulmonary Disease: Presented byDocumento25 pagineChronic Obstructive Pulmonary Disease: Presented byChinni 12599Nessuna valutazione finora
- Asthma Patient ProfileDocumento8 pagineAsthma Patient ProfileGlenn Asuncion PagaduanNessuna valutazione finora
- Checklists of Respiratory System AssessmentDocumento22 pagineChecklists of Respiratory System AssessmentDhrumini PatelNessuna valutazione finora
- Eye ExaminationDocumento23 pagineEye Examinationcynthia167Nessuna valutazione finora
- Congestive Cardiac Failure by NeetaDocumento26 pagineCongestive Cardiac Failure by NeetaNeeta AnandaNessuna valutazione finora
- DVT Guide: Symptoms, Risks and TreatmentDocumento9 pagineDVT Guide: Symptoms, Risks and TreatmentGladys YaresNessuna valutazione finora
- Peripheral Artery Disease: Nikhil Vaishnav M.Sc. (Nursing)Documento70 paginePeripheral Artery Disease: Nikhil Vaishnav M.Sc. (Nursing)Dimpal ChoudharyNessuna valutazione finora
- Complete Physical Examination ChecklistDocumento5 pagineComplete Physical Examination Checklistapi-641836481Nessuna valutazione finora
- Respiratory Assessment FindingsDocumento197 pagineRespiratory Assessment Findingsannatw100% (2)
- CPRDocumento41 pagineCPRKusumNessuna valutazione finora
- Managing COPD: Nursing Care for Breathing Issues, Nutrition, Infection RiskDocumento2 pagineManaging COPD: Nursing Care for Breathing Issues, Nutrition, Infection RiskAl RizkyNessuna valutazione finora
- DKA: Diagnosis and Treatment of Diabetic KetoacidosisDocumento20 pagineDKA: Diagnosis and Treatment of Diabetic KetoacidosisHUSSAIN NAZEESHANessuna valutazione finora
- Cardiac ComplicationDocumento12 pagineCardiac ComplicationResa ShotsNessuna valutazione finora
- Acute and Chronic Renal Failure Assessment and ManagementDocumento76 pagineAcute and Chronic Renal Failure Assessment and Managementphoenix180100% (1)
- DKA Study GroupDocumento24 pagineDKA Study GroupAqila MumtazNessuna valutazione finora
- Burn NursingDocumento13 pagineBurn NursingAndi sutandi50% (2)
- Rheumatic Heart DiseaseDocumento22 pagineRheumatic Heart DiseasemajdNessuna valutazione finora
- Common Ecg Abnormalities PDFDocumento2 pagineCommon Ecg Abnormalities PDFRonNessuna valutazione finora
- Cardiac Dysrhythmias: Mrs. D. Melba Sahaya Sweety M.SC Nursing GimsarDocumento60 pagineCardiac Dysrhythmias: Mrs. D. Melba Sahaya Sweety M.SC Nursing GimsarD. Melba S.S ChinnaNessuna valutazione finora
- Thyroid Status Examination OSCE GuideDocumento20 pagineThyroid Status Examination OSCE GuideemmaNessuna valutazione finora
- Miconium Aspiration SyndromeDocumento19 pagineMiconium Aspiration SyndromeEnna PaulaNessuna valutazione finora
- Cardiac Case StudyDocumento44 pagineCardiac Case StudyNatalia Bernard100% (1)
- Chest Pain Non TraumaDocumento45 pagineChest Pain Non TraumaTita LuthfiaNessuna valutazione finora
- Basic Respiratory Mechanics: Ventilation, Diffusion, and Gas ExchangeDocumento36 pagineBasic Respiratory Mechanics: Ventilation, Diffusion, and Gas ExchangeRizqi Luqmanul HakimNessuna valutazione finora
- Pulmonary Function TestDocumento57 paginePulmonary Function TestDeepika PatelNessuna valutazione finora
- Generic Name Therapeutic Classification Pharmacologic ClassificationDocumento3 pagineGeneric Name Therapeutic Classification Pharmacologic ClassificationAnselle CasilNessuna valutazione finora
- Case Presentation On Recurrent PULMONARY EMBOLISMDocumento14 pagineCase Presentation On Recurrent PULMONARY EMBOLISMAkas RehmanNessuna valutazione finora
- Transitional Care Case Study-Pulling It All TogetherDocumento13 pagineTransitional Care Case Study-Pulling It All TogethermatthewNessuna valutazione finora
- Case Study About: Cardiac Failure and Pulmonary EdemaDocumento32 pagineCase Study About: Cardiac Failure and Pulmonary EdemaIan Simon DorojaNessuna valutazione finora
- ShockDocumento7 pagineShockmara5140Nessuna valutazione finora
- NIV Fs 9108147 e 1911 1 PDFDocumento4 pagineNIV Fs 9108147 e 1911 1 PDFliuchenshitaoNessuna valutazione finora
- Nursing Process 3Documento10 pagineNursing Process 3Shubhra Sheoran100% (1)
- Insulin AdministrationDocumento8 pagineInsulin AdministrationskybluealiNessuna valutazione finora
- Congestive Heart FailureDocumento19 pagineCongestive Heart FailureIlavenil PanduranganNessuna valutazione finora
- Congestive Heart FailureDocumento86 pagineCongestive Heart FailureNabeel ShahzadNessuna valutazione finora
- Advanced Cardiac ProcedureDocumento9 pagineAdvanced Cardiac ProcedureSachin DwivediNessuna valutazione finora
- Cardio Vascular Assessment: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingDocumento46 pagineCardio Vascular Assessment: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingmeghanaNessuna valutazione finora
- Dissiminated Intravascular Coagulation PathoDocumento2 pagineDissiminated Intravascular Coagulation Pathoapi-341263362Nessuna valutazione finora
- Ventricular Fibrillation/ Pulseless Ventricular Tachycardia AlgorithmDocumento2 pagineVentricular Fibrillation/ Pulseless Ventricular Tachycardia AlgorithmsafasayedNessuna valutazione finora
- Nursing Management of Congestive Heart FailureDocumento37 pagineNursing Management of Congestive Heart FailurePierre Aseron ManuelNessuna valutazione finora
- Care of Patient With TPM Slide PresentationDocumento16 pagineCare of Patient With TPM Slide PresentationirzehronNessuna valutazione finora
- GCS Assessment Aid English PDFDocumento1 paginaGCS Assessment Aid English PDFSila OntitaNessuna valutazione finora
- Physical Examination: Binal Joshi Assistant Professor Child Health Nursing Manikaka Topawala Institute of NursingDocumento101 paginePhysical Examination: Binal Joshi Assistant Professor Child Health Nursing Manikaka Topawala Institute of NursingBinal JoshiNessuna valutazione finora
- United Doctors Hospital Nurses Handover ReportDocumento20 pagineUnited Doctors Hospital Nurses Handover ReportANNETTE GUEVARRANessuna valutazione finora
- Emergency Drugs KathDocumento29 pagineEmergency Drugs Kathmajin655Nessuna valutazione finora
- Cushings SyndromeDocumento51 pagineCushings SyndromeTina TalmadgeNessuna valutazione finora
- Cardiac Rehab After CABGDocumento31 pagineCardiac Rehab After CABGShefali SharmaNessuna valutazione finora
- ICU Scoring Systems A Complete Guide - 2020 EditionDa EverandICU Scoring Systems A Complete Guide - 2020 EditionNessuna valutazione finora
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Neck LumpDocumento18 pagineNeck LumpJosh BurkeNessuna valutazione finora
- Antibiotics Study Guide 2017Documento13 pagineAntibiotics Study Guide 2017Josh BurkeNessuna valutazione finora
- Central Nervous System Tumours OverviewDocumento35 pagineCentral Nervous System Tumours OverviewJosh BurkeNessuna valutazione finora
- Blood Sugars - DiabetesDocumento31 pagineBlood Sugars - DiabetesJosh BurkeNessuna valutazione finora
- Physiology of Pregnancy - Pre-Eclampsia DiabetesDocumento34 paginePhysiology of Pregnancy - Pre-Eclampsia DiabetesJosh BurkeNessuna valutazione finora
- Block 5 Anatomy Seminar 1 Perineum MG - 5MAY2016Documento22 pagineBlock 5 Anatomy Seminar 1 Perineum MG - 5MAY2016Josh BurkeNessuna valutazione finora
- Joint British Diabetes Societies Inpatient Care Group - The Management of Diabetic Ketoacidosis in Adults - Pathway PosterDocumento1 paginaJoint British Diabetes Societies Inpatient Care Group - The Management of Diabetic Ketoacidosis in Adults - Pathway PosterAllison Nadine MarchandNessuna valutazione finora
- Abdo PainDocumento35 pagineAbdo PainJosh BurkeNessuna valutazione finora
- Niel Gows Lament For The Death of His Second Wife-Mandolin-Tab PDFDocumento1 paginaNiel Gows Lament For The Death of His Second Wife-Mandolin-Tab PDFJosh BurkeNessuna valutazione finora
- Physical Exam Reasons: Hands, Eyes, and MoreDocumento1 paginaPhysical Exam Reasons: Hands, Eyes, and MoreJosh BurkeNessuna valutazione finora
- Hyponatraemia QuizDocumento4 pagineHyponatraemia QuizJosh BurkeNessuna valutazione finora
- Professional Behaviour and Fitness To Practise 0816.PDF 66085925Documento84 pagineProfessional Behaviour and Fitness To Practise 0816.PDF 66085925Josh BurkeNessuna valutazione finora
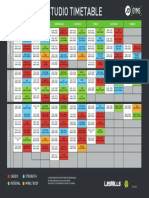
- Coventry Timetable SEP16Documento1 paginaCoventry Timetable SEP16Josh BurkeNessuna valutazione finora
- LVSDDocumento6 pagineLVSDJosh BurkeNessuna valutazione finora
- MurmursDocumento2 pagineMurmursJosh Burke100% (1)
- PoCUS Program 1016Documento3 paginePoCUS Program 1016Josh BurkeNessuna valutazione finora
- Leclair 6 Sonatas Op.3 Nos 4 6Documento25 pagineLeclair 6 Sonatas Op.3 Nos 4 6Josh Burke100% (2)
- Bruni 6 Duettini Op.34Documento24 pagineBruni 6 Duettini Op.34Josh BurkeNessuna valutazione finora
- R IntroDocumento105 pagineR Introtp2006sterNessuna valutazione finora
- Softship SeabearDocumento1 paginaSoftship SeabearJosh BurkeNessuna valutazione finora
- Anxiety and Panic Attacks: Symptoms and Risk FactorsDocumento11 pagineAnxiety and Panic Attacks: Symptoms and Risk FactorsJosh BurkeNessuna valutazione finora
- Symptoms and Risk FactorsDocumento4 pagineSymptoms and Risk FactorsJosh BurkeNessuna valutazione finora
- Adult1 16-25 - 04sep16Documento1 paginaAdult1 16-25 - 04sep16Josh BurkeNessuna valutazione finora
- R IntroDocumento105 pagineR Introtp2006sterNessuna valutazione finora
- Handel HWV348 50hha - Violin1Documento13 pagineHandel HWV348 50hha - Violin1Josh BurkeNessuna valutazione finora
- Crockpot RecipiesDocumento45 pagineCrockpot RecipiescpantsulaNessuna valutazione finora
- Barclays Money Skills Toolkit - Aged 16 - 25Documento107 pagineBarclays Money Skills Toolkit - Aged 16 - 25Josh BurkeNessuna valutazione finora
- Beriot Method Part 1Documento78 pagineBeriot Method Part 1Caitriona HollandNessuna valutazione finora
- Bladder StonesDocumento20 pagineBladder StonesRiean AuliaNessuna valutazione finora
- Soap Note Template 33Documento3 pagineSoap Note Template 33Rafael G. Garcia SanchezNessuna valutazione finora
- Asian Music Research - J.C GarciaDocumento5 pagineAsian Music Research - J.C GarciaJomel GarciaNessuna valutazione finora
- BSSP Course DescriptionsDocumento3 pagineBSSP Course DescriptionsJilliane LagusNessuna valutazione finora
- Health & Nutrition Classification of FoodDocumento10 pagineHealth & Nutrition Classification of Foodg20kpNessuna valutazione finora
- Drug StudyDocumento5 pagineDrug StudyRai D. MacapantonNessuna valutazione finora
- Peptic UlcerDocumento4 paginePeptic UlcerEris Abdul AzizNessuna valutazione finora
- Psychoeducation as Evidence-Based Practice: A Review of its Applications Across SettingsDocumento21 paginePsychoeducation as Evidence-Based Practice: A Review of its Applications Across SettingsEduardo Aguirre DávilaNessuna valutazione finora
- Paper On Intergenerational TraumaDocumento13 paginePaper On Intergenerational TraumaEdith G.LebelNessuna valutazione finora
- AmenorrheaDocumento41 pagineAmenorrheaDewi Felayati Gusni100% (2)
- The EyeDocumento8 pagineThe Eyezyrine jhen100% (1)
- Cyanide PoisoningDocumento5 pagineCyanide Poisoningriz04_fortitudessa5178Nessuna valutazione finora
- Kidney Stones, UTI, Bladder Control: Causes, Symptoms, Prevention/TITLEDocumento24 pagineKidney Stones, UTI, Bladder Control: Causes, Symptoms, Prevention/TITLEIsabella Alycia Lomibao100% (1)
- C Perfringens Cladosporium SPP - PDFDocumento21 pagineC Perfringens Cladosporium SPP - PDFEman QasmNessuna valutazione finora
- PT of The Shoulder PDFDocumento573 paginePT of The Shoulder PDFMuhammad Salman AzimNessuna valutazione finora
- 2015 Budget Supply PlanDocumento65 pagine2015 Budget Supply PlanGetu BogaleNessuna valutazione finora
- Pooja - 1Documento61 paginePooja - 1Shobhit GoswamiNessuna valutazione finora
- Personal Trainer Magazine PDFDocumento54 paginePersonal Trainer Magazine PDFdixieakerszNessuna valutazione finora
- Neonatal Resuscitation AlgorithmDocumento1 paginaNeonatal Resuscitation Algorithmpalembang2015Nessuna valutazione finora
- Mental Health and Mental IllnessesDocumento108 pagineMental Health and Mental IllnessesVictoria VellaNessuna valutazione finora
- CP - Hemophilia 2Documento40 pagineCP - Hemophilia 2Reezka PutraNessuna valutazione finora
- Abnormal-Uterine-Bleeding Case StudyDocumento57 pagineAbnormal-Uterine-Bleeding Case StudyOneForAll :100% (1)
- Friedberg Wilt 2010 CT and MetaphorsDocumento16 pagineFriedberg Wilt 2010 CT and MetaphorsAlexandra HuhNessuna valutazione finora
- Harbor City Behavioral Health Center BrochureDocumento2 pagineHarbor City Behavioral Health Center BrochureAlfredo GonzálezNessuna valutazione finora
- Bleomycin Monograph 1dec2014Documento10 pagineBleomycin Monograph 1dec2014cmeytasNessuna valutazione finora
- Preventing Illness and Living With Ill HealthDocumento11 paginePreventing Illness and Living With Ill HealthMonique MavronicolasNessuna valutazione finora
- Cultivation of Super Food Spirulina Blue-Green Algae An AgribusinessDocumento8 pagineCultivation of Super Food Spirulina Blue-Green Algae An AgribusinessRupesh Kumar100% (1)
- HISTORY OF ORTHODONTICSDocumento185 pagineHISTORY OF ORTHODONTICSvelangni83% (6)
- Pentagon Reviewer Med SurgDocumento31 paginePentagon Reviewer Med SurgKathy Real VillsNessuna valutazione finora
- Addressing Cognition Poster 36x42Documento1 paginaAddressing Cognition Poster 36x42api-262531856Nessuna valutazione finora