Potrebbero piacerti anche
- Pathophysiology of Rheumatic Heart DiseaseDocumento3 paginePathophysiology of Rheumatic Heart DiseaseXtiaR85% (13)
- Operative Dentistry in the Phantom LabDa EverandOperative Dentistry in the Phantom LabValutazione: 5 su 5 stelle5/5 (1)
- Pit and Fissure SealantsDocumento34 paginePit and Fissure SealantsSamridhi SrivastavaNessuna valutazione finora
- Failures and ManagementDocumento25 pagineFailures and Managementitsme5432100% (1)
- Seminar 6 - Dental CementsDocumento114 pagineSeminar 6 - Dental Cementsaziz2007100% (1)
- Fixed Partial Denture 1Documento93 pagineFixed Partial Denture 1Docshiv Dent100% (4)
- Zinc Polycarboxylate CementDocumento18 pagineZinc Polycarboxylate Cementmerobabu100% (1)
- Dental CementsDocumento208 pagineDental CementsAkriti Goel33% (3)
- Basic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionDa EverandBasic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionNessuna valutazione finora
- Dental Materials 2Documento11 pagineDental Materials 2AnilNessuna valutazione finora
- Dental Materials IVDocumento11 pagineDental Materials IVkevin1678100% (1)
- Synthetic Resins in ProsthodonticsDocumento40 pagineSynthetic Resins in Prosthodonticssankar100% (1)
- Dental MaterialsDocumento33 pagineDental Materialskevin1678Nessuna valutazione finora
- Denture Base MaterialDocumento100 pagineDenture Base Materialpbhu1Nessuna valutazione finora
- Space MaintainerDocumento36 pagineSpace MaintainerDenis KimNessuna valutazione finora
- Dental WaxesDocumento7 pagineDental WaxesNurul IzzatiNessuna valutazione finora
- CHAPTER 1 Manual OperativeDocumento27 pagineCHAPTER 1 Manual OperativeCassie Von PeenqNessuna valutazione finora
- Dental AmalgamDocumento30 pagineDental Amalgamshaniaz19785112Nessuna valutazione finora
- Management of Discoloured Teeth: Presented By: Amisha Jain M.D.S II YearDocumento44 pagineManagement of Discoloured Teeth: Presented By: Amisha Jain M.D.S II YearANUBHANessuna valutazione finora
- Glass Ionomer CementDocumento57 pagineGlass Ionomer CementAmniAzmi100% (1)
- Dental AmalgamDocumento182 pagineDental AmalgamPayal Batavia100% (1)
- Tests For Biocompatibility of Dental MaterialsDocumento151 pagineTests For Biocompatibility of Dental MaterialsDevanshi SharmaNessuna valutazione finora
- L2-Dental Materials in DENT3020Documento49 pagineL2-Dental Materials in DENT3020Trebor ErebutNessuna valutazione finora
- Rotary EndodonticsDocumento61 pagineRotary EndodonticsVijayendra kamathNessuna valutazione finora
- Conservative DentistryDocumento6 pagineConservative DentistryAbdallah Essam Al-ZireeniNessuna valutazione finora
- Denture Base ResinsDocumento70 pagineDenture Base ResinsSusovan Giri100% (1)
- Silicate CementDocumento20 pagineSilicate CementMayuri Naik67% (3)
- Acid EtchDocumento46 pagineAcid EtchSandeep Reddy100% (1)
- Dental Material SlidesDocumento73 pagineDental Material SlidesAri IsmaelNessuna valutazione finora
- Physical Properties of Dental MaterialsDocumento87 paginePhysical Properties of Dental MaterialsManiBernardH100% (1)
- Lecture 18 & 19 - Abrasives and Temporary Crowns Material (Slides)Documento57 pagineLecture 18 & 19 - Abrasives and Temporary Crowns Material (Slides)JustDen09Nessuna valutazione finora
- Dental Cements: BY Pranalika Kanojiya Mds 1 YearDocumento128 pagineDental Cements: BY Pranalika Kanojiya Mds 1 Yearpranalika .................Nessuna valutazione finora
- Denure Base ResinDocumento94 pagineDenure Base ResinVishnu S Pattath100% (1)
- Sample Presentation - Denture Base MaterialsDocumento99 pagineSample Presentation - Denture Base MaterialsDrnisanth100% (1)
- Zinc Poly Carboxylate CementDocumento41 pagineZinc Poly Carboxylate CementASHWINI ATHULNessuna valutazione finora
- Dental Materials Sample PDFDocumento30 pagineDental Materials Sample PDFAnil Sukumaran100% (1)
- Model and Die Materials Final 1Documento22 pagineModel and Die Materials Final 1drkarthikmds100% (1)
- Crown and Bridge: A) 1. Complete Coverage (Full Veneer Crown) : ItDocumento5 pagineCrown and Bridge: A) 1. Complete Coverage (Full Veneer Crown) : ItRihan RihanNessuna valutazione finora
- Single Vs Multiple Visits in PulpectomyDocumento7 pagineSingle Vs Multiple Visits in PulpectomyHudh HudNessuna valutazione finora
- Umbrella Effect of GICDocumento11 pagineUmbrella Effect of GICLavanya Priya50% (4)
- Dental ProductsDocumento55 pagineDental ProductsIshtiaq Ahmed80% (5)
- Composite RestorationsDocumento66 pagineComposite Restorationsviansabah100% (1)
- Glass Ionomer Cement PolyalkenoatesDocumento26 pagineGlass Ionomer Cement PolyalkenoatesArifa parveenNessuna valutazione finora
- Recent Advances in Composites PDFDocumento7 pagineRecent Advances in Composites PDFShriya Shahu100% (1)
- Plaque and BiofilmDocumento59 paginePlaque and BiofilmGorremuchu Srinivas100% (2)
- Introduction of Dental Material ScienceDocumento40 pagineIntroduction of Dental Material ScienceskyNessuna valutazione finora
- GicDocumento75 pagineGicNihar Arya100% (1)
- Role of Saliva in Dental CariesDocumento29 pagineRole of Saliva in Dental Carieskhush sidhu100% (1)
- Rationale of Endodontic TreatmentDocumento45 pagineRationale of Endodontic TreatmentAmy Rita0% (1)
- Impression MaterialsDocumento60 pagineImpression Materialsمحمد احمد محمدNessuna valutazione finora
- Toothseperationmatrixwedges 140518082259 Phpapp01Documento74 pagineToothseperationmatrixwedges 140518082259 Phpapp01hazeemmegahedNessuna valutazione finora
- Dental CompositesDocumento52 pagineDental CompositesMavic Mahinay100% (1)
- Essentials of Oral MedicineDocumento389 pagineEssentials of Oral MedicineKishendran R GanandranNessuna valutazione finora
- Microbiology Aspect in EndodonticsDocumento80 pagineMicrobiology Aspect in Endodonticswhussien7376100% (1)
- New Microsoft PowerPoint PresentationDocumento158 pagineNew Microsoft PowerPoint PresentationSutapa Roy100% (1)
- Resin Cememt - 2Documento108 pagineResin Cememt - 2Shrinidhi R PoonjaNessuna valutazione finora
- Abrasive Agents in DentistryDocumento38 pagineAbrasive Agents in Dentistryjohn mwambu100% (1)
- Intracanal MedicamentsDocumento106 pagineIntracanal Medicamentsrolly_jatin100% (3)
- Denture Base MaterialsDocumento27 pagineDenture Base MaterialsAmmar Al ZoubiNessuna valutazione finora
- Dental BursDocumento28 pagineDental Burstarekrabi0% (1)
- UndreloDocumento3 pagineUndrelobabaNessuna valutazione finora
- Project Management Dashboard TemplateDocumento1 paginaProject Management Dashboard TemplatebabaNessuna valutazione finora
- Project Management Dashboard TemplateDocumento1 paginaProject Management Dashboard TemplatebabaNessuna valutazione finora
- Sample LettersDocumento8 pagineSample LettersaliNessuna valutazione finora
- Best Letter FormateDocumento1 paginaBest Letter FormatebabaNessuna valutazione finora
- Business LetterDocumento3 pagineBusiness LetterbabaNessuna valutazione finora
- BBBBBBGDocumento1 paginaBBBBBBGbabaNessuna valutazione finora
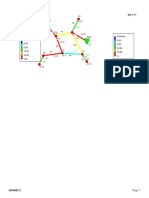
- Heat Map ReportingDocumento1 paginaHeat Map ReportingAHmeD AbdelrahmanNessuna valutazione finora
- Pressure 0.00 5.00 20.00 26.00 M Flow 0.00 5.00 10.00 20.00 LPSDocumento1 paginaPressure 0.00 5.00 20.00 26.00 M Flow 0.00 5.00 10.00 20.00 LPSbabaNessuna valutazione finora
- Pressure 0.00 5.00 20.00 26.00 M Flow 0.00 5.00 10.00 20.00 LPSDocumento1 paginaPressure 0.00 5.00 20.00 26.00 M Flow 0.00 5.00 10.00 20.00 LPSbabaNessuna valutazione finora
- Module6 - MBIE - Earthquake GuidanceDocumento80 pagineModule6 - MBIE - Earthquake GuidanceDoralba V NolanNessuna valutazione finora
- Code of EthicsDocumento1 paginaCode of EthicsUsman034Nessuna valutazione finora
- Ms ProjectDocumento1 paginaMs ProjectbabaNessuna valutazione finora
- ScheduleDocumento1 paginaSchedulebabaNessuna valutazione finora
- 2023-24 SR - Super60 (Incoming) STERLING Batch CHEMISTRY Teaching & Test Schedule Code@03!04!2023Documento16 pagine2023-24 SR - Super60 (Incoming) STERLING Batch CHEMISTRY Teaching & Test Schedule Code@03!04!2023K R I S H100% (1)
- Grade-9-Parallel-Test-LAS-1.2 CDocumento2 pagineGrade-9-Parallel-Test-LAS-1.2 CArth Renier MinaNessuna valutazione finora
- The Company - MicroDocumento2 pagineThe Company - MicroMai Hương QuỳnhNessuna valutazione finora
- Sales Order Process - Key Steps, Attributes and Concepts - v7Documento25 pagineSales Order Process - Key Steps, Attributes and Concepts - v7bob bluhmNessuna valutazione finora
- DT-M Datasheet Vertex Ne19r en 2022 Pa1 Web Ne19r 2022pa1 en 20220916Documento2 pagineDT-M Datasheet Vertex Ne19r en 2022 Pa1 Web Ne19r 2022pa1 en 20220916Producto ITICCOLNessuna valutazione finora
- Selection and Ranking of Rail Vehicle Components For Optimal Lightweighting Using Composite MaterialsDocumento14 pagineSelection and Ranking of Rail Vehicle Components For Optimal Lightweighting Using Composite MaterialsAwan AJaNessuna valutazione finora
- Pneumatic Oscillator Valve - Pneumatic Controls - Impulse Automation LTDDocumento3 paginePneumatic Oscillator Valve - Pneumatic Controls - Impulse Automation LTDDindin NajmudinNessuna valutazione finora
- TZ150-03 Service Manual - ChopperDocumento42 pagineTZ150-03 Service Manual - ChopperMax Dean Araújo FernandesNessuna valutazione finora
- Wifpl Qap 2019-20-058 Rev 00 Konecranes 18crnimo7 6 SignedDocumento2 pagineWifpl Qap 2019-20-058 Rev 00 Konecranes 18crnimo7 6 SignedDeepak HoleNessuna valutazione finora
- Public Places 9 & 10Documento2 paginePublic Places 9 & 10kaka udinNessuna valutazione finora
- Vision Medilink Product DetailsDocumento4 pagineVision Medilink Product DetailsRaj SekarNessuna valutazione finora
- Personal Loan For JoiningDocumento3 paginePersonal Loan For JoiningAzim SengalNessuna valutazione finora
- Material Safety Data Sheet Glyphosate 5.4Documento5 pagineMaterial Safety Data Sheet Glyphosate 5.4Ahfi Rizqi FajrinNessuna valutazione finora
- Steri - Cycle I 160 New GenDocumento16 pagineSteri - Cycle I 160 New GenLEO AROKYA DASSNessuna valutazione finora
- Employement ExchangeDocumento22 pagineEmployement ExchangeNeelam ThakurNessuna valutazione finora
- Ielts ReadingDocumento7 pagineIelts ReadingTrọng Nguyễn DuyNessuna valutazione finora
- Wastewater Treatment Lab TestDocumento8 pagineWastewater Treatment Lab TesthuyNessuna valutazione finora
- Wind Energy Wind Is Generated As The Fluid and Gaseous Parts of The Atmosphere Move Across The Surface of The EarthDocumento3 pagineWind Energy Wind Is Generated As The Fluid and Gaseous Parts of The Atmosphere Move Across The Surface of The EarthEphraim TermuloNessuna valutazione finora
- Chapter 8 Sensation and PerceptionDocumento66 pagineChapter 8 Sensation and Perceptionapi-726122866Nessuna valutazione finora
- AscindiaDocumento16 pagineAscindiaHeeman TrivediNessuna valutazione finora
- Potential Use of Probiotics: Ekachai ChukeatiroteDocumento8 paginePotential Use of Probiotics: Ekachai ChukeatiroteDanu EffendiNessuna valutazione finora
- TympanometerDocumento12 pagineTympanometerAli ImranNessuna valutazione finora
- 250 Watt Solar Panel SpecificationsDocumento2 pagine250 Watt Solar Panel Specificationsfopoku2k20% (1)
- Effect of Educational Environment On Personality and Adjustment of Female Students Studying in Colleges of UttarakhandDocumento5 pagineEffect of Educational Environment On Personality and Adjustment of Female Students Studying in Colleges of UttarakhandESSENCE - International Journal for Environmental Rehabilitation and ConservaionNessuna valutazione finora
- A Guide To Patient Medication Review: September 2003Documento33 pagineA Guide To Patient Medication Review: September 2003Muhamad GunturNessuna valutazione finora
- POCSO Handbook-CombinedDocumento39 paginePOCSO Handbook-CombinedInspector General of Police South ZoneNessuna valutazione finora
- 4 26 12Documento9 pagine4 26 12stevenscreekNessuna valutazione finora
- Carcinoma of Prostate: Dr. Saadat Hashmi Consultant UrologistDocumento48 pagineCarcinoma of Prostate: Dr. Saadat Hashmi Consultant UrologistMuhammad ArsalNessuna valutazione finora