Potrebbero piacerti anche
- Male Reproductive Organs 2018Documento80 pagineMale Reproductive Organs 2018yasrul izad100% (1)
- Anatomy of Circulatory SystemDocumento56 pagineAnatomy of Circulatory SystemLina Wijaya100% (1)
- Femoral Sheath and Femoral TriangleDocumento23 pagineFemoral Sheath and Femoral TriangleSamiha Haq100% (2)
- Empirical First Line AntibioticsDocumento1 paginaEmpirical First Line Antibioticsdiati zahrainiNessuna valutazione finora
- Osteology of The Upper Limb LectureDocumento40 pagineOsteology of The Upper Limb LectureFavour OnyeaboNessuna valutazione finora
- Colorectal MalignancyDocumento108 pagineColorectal MalignancySatishht SatishNessuna valutazione finora
- Popliteal Fossa and LegDocumento40 paginePopliteal Fossa and LegRaj Shekhar SinghNessuna valutazione finora
- Nose & Paranasal Sinuses 2018Documento63 pagineNose & Paranasal Sinuses 2018yasrul izadNessuna valutazione finora
- Masters of physiotherapy introduce thoracic bonesDocumento30 pagineMasters of physiotherapy introduce thoracic bonesShikha SagarNessuna valutazione finora
- Acupuncture, Trigger Points and Musculoskeletal Pain - Peter E. BaldryDocumento378 pagineAcupuncture, Trigger Points and Musculoskeletal Pain - Peter E. Baldrygerkenp100% (6)
- Foot and Ankle Bones and JointsDocumento43 pagineFoot and Ankle Bones and Jointshannah murphyNessuna valutazione finora
- Blood Cells and Its Types With FunctionsDocumento5 pagineBlood Cells and Its Types With Functionskaleb16_2Nessuna valutazione finora
- Cardiac CycleDocumento31 pagineCardiac CycleAdwaitha KrNessuna valutazione finora
- Anatomy of Esophagus and StomachDocumento65 pagineAnatomy of Esophagus and Stomachmackiecc100% (2)
- Cardiac Cycle: Prepared By: Mineshkumar Prajapati Roll No: 05 Biomedical Science (2021-22)Documento21 pagineCardiac Cycle: Prepared By: Mineshkumar Prajapati Roll No: 05 Biomedical Science (2021-22)minesh prajapatiNessuna valutazione finora
- Dr. Reynaldo V. Lopez Senior Lecturer Department of AnatomyDocumento55 pagineDr. Reynaldo V. Lopez Senior Lecturer Department of AnatomyMohammad AliNessuna valutazione finora
- Unit 6 Part 2 Thoracic CavityDocumento56 pagineUnit 6 Part 2 Thoracic CavitySiraj ShiferawNessuna valutazione finora
- Anterior Triangle of The Neck IIDocumento49 pagineAnterior Triangle of The Neck IIvrajNessuna valutazione finora
- Femoral Region, Anterior and Medial Compartments of The ThighDocumento49 pagineFemoral Region, Anterior and Medial Compartments of The ThighNolanNessuna valutazione finora
- Joints of Lower Limb 2017Documento77 pagineJoints of Lower Limb 2017yasrul izadNessuna valutazione finora
- Joints of Lower Limb 2017Documento77 pagineJoints of Lower Limb 2017yasrul izadNessuna valutazione finora
- ANKLE JOINT &joints of FootDocumento35 pagineANKLE JOINT &joints of Foothhaanniiss3870Nessuna valutazione finora
- Ascending Descending TractsDocumento46 pagineAscending Descending Tractsyasrul izad100% (3)
- Peritoneum: General FeaturesDocumento92 paginePeritoneum: General FeaturestuhinsinghNessuna valutazione finora
- Hafizah Binti Mohd Hoshni Musculoskeletal Anatomy Skeleton of The ThoraxDocumento28 pagineHafizah Binti Mohd Hoshni Musculoskeletal Anatomy Skeleton of The ThoraxhafizahhoshniNessuna valutazione finora
- Large Blood Vessels of The GutDocumento61 pagineLarge Blood Vessels of The GutpoojaNessuna valutazione finora
- Kuliah Spine TraumaDocumento91 pagineKuliah Spine TraumaEvi MaisyariNessuna valutazione finora
- Upper Limb 1Documento14 pagineUpper Limb 1faraNessuna valutazione finora
- Mammary Gland Structure and DevelopmentDocumento22 pagineMammary Gland Structure and DevelopmentAaronMaroonFiveNessuna valutazione finora
- 07 Gall BladderDocumento67 pagine07 Gall BladdershamsorahNessuna valutazione finora
- 16-Genital ProlapseDocumento37 pagine16-Genital Prolapseapi-3703352Nessuna valutazione finora
- Basal Ganglia & CerebellumDocumento77 pagineBasal Ganglia & Cerebellumyasrul izadNessuna valutazione finora
- The Acupuncture Prescription:: A Holistic Approach to HealthDa EverandThe Acupuncture Prescription:: A Holistic Approach to HealthNessuna valutazione finora
- COURSE AND BRANCHES OF THE MAXILLARY NERVEDocumento26 pagineCOURSE AND BRANCHES OF THE MAXILLARY NERVEHanaMajeedNessuna valutazione finora
- Peritoneum and Peritoneal CavityDocumento26 paginePeritoneum and Peritoneal CavitytuhinsinghNessuna valutazione finora
- Genital ProlapseDocumento9 pagineGenital Prolapsesher singhNessuna valutazione finora
- Thursday, April 09, 2009 4:45 PMDocumento266 pagineThursday, April 09, 2009 4:45 PMkcs2012Nessuna valutazione finora
- Circumflex Scapular: Dorsum of Thoracodorsal: Latissmus DorsiDocumento4 pagineCircumflex Scapular: Dorsum of Thoracodorsal: Latissmus Dorsispeedy.catNessuna valutazione finora
- HSB - Head and Scalp AnatomyDocumento19 pagineHSB - Head and Scalp AnatomyRaki IliganNessuna valutazione finora
- Monoclonal Antibodies and Engineered AntibodiesDocumento24 pagineMonoclonal Antibodies and Engineered AntibodiesMunawar AliNessuna valutazione finora
- Abdominal WallDocumento56 pagineAbdominal WallAHMAD KHANNessuna valutazione finora
- Comprehensive Physical AssessmentDocumento2 pagineComprehensive Physical AssessmentJan Christian Dayto79% (33)
- Large IntestineDocumento50 pagineLarge Intestinemex Gbrekorkos100% (1)
- The Neurovascular Bundle of The Anterior Compartment ofDocumento30 pagineThe Neurovascular Bundle of The Anterior Compartment ofAnnapurna Bose100% (2)
- Cat Muscles and O.I.A.: Body Region Muscle Origin Insertion ActionDocumento5 pagineCat Muscles and O.I.A.: Body Region Muscle Origin Insertion ActioneumarasiganNessuna valutazione finora
- Thoracic Wall.Documento48 pagineThoracic Wall.Shimmering MoonNessuna valutazione finora
- Thoracic CageDocumento30 pagineThoracic CageLizz MarieNessuna valutazione finora
- Anatomy, Lecture 9, Abdominal WallDocumento22 pagineAnatomy, Lecture 9, Abdominal WallAli Al-QudsiNessuna valutazione finora
- Anatomy of Lung, Pleura, Surface MarkingDocumento22 pagineAnatomy of Lung, Pleura, Surface MarkingSandhya SureshNessuna valutazione finora
- Nerves of Lower Limb and Their Injuries: Learning ObjectivesDocumento8 pagineNerves of Lower Limb and Their Injuries: Learning ObjectivesUloko ChristopherNessuna valutazione finora
- Lumbosacral PlexusDocumento3 pagineLumbosacral Plexusgehaoi4Nessuna valutazione finora
- 7th Week Femoral Sheath, Femoral Triangle and Adductor CanalDocumento17 pagine7th Week Femoral Sheath, Femoral Triangle and Adductor CanalShah NawazNessuna valutazione finora
- Thorax AllDocumento174 pagineThorax Allravindra sharmaNessuna valutazione finora
- Bones of The Lower LimbDocumento15 pagineBones of The Lower Limbyachiru121Nessuna valutazione finora
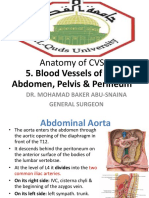
- Anatomy of CVS: 5. Blood Vessels of The Abdomen, Pelvis & PerineumDocumento30 pagineAnatomy of CVS: 5. Blood Vessels of The Abdomen, Pelvis & Perineumsultan khabeebNessuna valutazione finora
- Abdominal Cavity: Peritoneum & GITDocumento32 pagineAbdominal Cavity: Peritoneum & GITAli Al-QudsiNessuna valutazione finora
- Anatomy - Abdomen and PelvisDocumento46 pagineAnatomy - Abdomen and PelvisDr.G.Bhanu PrakashNessuna valutazione finora
- Borders: Teachmeseries LTDDocumento3 pagineBorders: Teachmeseries LTDlecturioNessuna valutazione finora
- Digestive System Power PointDocumento17 pagineDigestive System Power PointAlyssa Mae DapadapNessuna valutazione finora
- Urinary System (Anatomy and Physiology)Documento4 pagineUrinary System (Anatomy and Physiology)ALESSANDRA BALBONTIN PEGARIDONessuna valutazione finora
- Prof. Ghabisha Saif Posterior Abdominal Wall AnatomyDocumento36 pagineProf. Ghabisha Saif Posterior Abdominal Wall AnatomyAzizNessuna valutazione finora
- Surface Anatomy of the Head, Neck, and ThoraxDocumento57 pagineSurface Anatomy of the Head, Neck, and ThoraxLavina SofiaNessuna valutazione finora
- Nerves of Lower Limb and Their Injuries, S-Ii-Lm-0120Documento5 pagineNerves of Lower Limb and Their Injuries, S-Ii-Lm-0120Shab GeNessuna valutazione finora
- Fetal Pig AnatomyDocumento43 pagineFetal Pig Anatomymihai2242Nessuna valutazione finora
- 4rd Lecture - AbdomenDocumento26 pagine4rd Lecture - AbdomenZainab Jamal SiddiquiNessuna valutazione finora
- Anatomy of The Intercostal SpaceDocumento17 pagineAnatomy of The Intercostal Spacelovelyc95Nessuna valutazione finora
- Obturator NerveDocumento3 pagineObturator NerveDr santoshNessuna valutazione finora
- Anatomy of the Pituitary Fossa and Cavernous SinusDocumento6 pagineAnatomy of the Pituitary Fossa and Cavernous SinusAkhil BansalNessuna valutazione finora
- Heart Sounds - PracticalDocumento7 pagineHeart Sounds - Practicalshadapaaak100% (1)
- DiencephalonDocumento20 pagineDiencephalonyasrul izadNessuna valutazione finora
- Coronary Circulation 2018Documento52 pagineCoronary Circulation 2018yasrul izadNessuna valutazione finora
- Leg & Foot 2017Documento68 pagineLeg & Foot 2017yasrul izadNessuna valutazione finora
- Colon, Caecum & Appendix 2017Documento67 pagineColon, Caecum & Appendix 2017yasrul izad0% (1)
- Pancreas 2017Documento53 paginePancreas 2017yasrul izadNessuna valutazione finora
- Gluteal Region and Thigh 2017Documento79 pagineGluteal Region and Thigh 2017yasrul izadNessuna valutazione finora
- Colon, Caecum & Appendix 2017Documento67 pagineColon, Caecum & Appendix 2017yasrul izadNessuna valutazione finora
- Colon, Caecum & Appendix 2017Documento67 pagineColon, Caecum & Appendix 2017yasrul izadNessuna valutazione finora
- Cognitv EmphatyDocumento6 pagineCognitv EmphatyAndrea MenesesNessuna valutazione finora
- Keeler Ophthalmoscope Bulb and Retinoscope Bulb ModelsDocumento1 paginaKeeler Ophthalmoscope Bulb and Retinoscope Bulb ModelsEDRAES17Nessuna valutazione finora
- Kaloji Narayana Rao University Health Sciences College Allotment ListDocumento79 pagineKaloji Narayana Rao University Health Sciences College Allotment ListVivek GuptaNessuna valutazione finora
- Pacemaker - Mayo ClinicDocumento15 paginePacemaker - Mayo ClinicShehab AhmedNessuna valutazione finora
- CasestudynervoussystemDocumento2 pagineCasestudynervoussystemapi-265854240Nessuna valutazione finora
- Spironolactone Class Indications: 25MG TAB, 50Mg Tab, 100Mg TabDocumento2 pagineSpironolactone Class Indications: 25MG TAB, 50Mg Tab, 100Mg TabAhmad KusayiriNessuna valutazione finora
- FORMAT Discharge PlanDocumento5 pagineFORMAT Discharge PlanButchay LumbabNessuna valutazione finora
- Unit-V Chapter 20. Breathing and Exchange of Gases: Important PointsDocumento13 pagineUnit-V Chapter 20. Breathing and Exchange of Gases: Important PointsminaNessuna valutazione finora
- HSPK 2021Documento270 pagineHSPK 2021Sabrina Agustien SimanungkalitNessuna valutazione finora
- Unit 2Documento4 pagineUnit 2api-296199660Nessuna valutazione finora
- Pelvic Floor Exercises in The Elderly Irmina Nahon1Documento34 paginePelvic Floor Exercises in The Elderly Irmina Nahon1Anonymous C7H7wS6Nessuna valutazione finora
- Case Study of Mrs. WalkerDocumento4 pagineCase Study of Mrs. WalkerPreet ChahalNessuna valutazione finora
- Sage Char-Lee ResumeDocumento2 pagineSage Char-Lee Resumeapi-510197139Nessuna valutazione finora
- Influence of Cavity LiningDocumento7 pagineInfluence of Cavity Liningpatel keralNessuna valutazione finora
- Emotional Influences On Food Choice Sensory, Physiological andDocumento9 pagineEmotional Influences On Food Choice Sensory, Physiological andpanda_pandita22Nessuna valutazione finora
- Apotex Pharmachem Product ListDocumento2 pagineApotex Pharmachem Product Listমোঃ এমদাদুল হকNessuna valutazione finora
- PDF Created With Pdffactory Pro Trial Version: Page 1 of 3Documento3 paginePDF Created With Pdffactory Pro Trial Version: Page 1 of 3HindNessuna valutazione finora
- DR Wong Teck WeeipadDocumento2 pagineDR Wong Teck Weeipadtwwong68Nessuna valutazione finora
- Drug Study - VancomycinDocumento2 pagineDrug Study - VancomycinKhatlen BagaresNessuna valutazione finora
- Klucel - Varnostni List PDFDocumento4 pagineKlucel - Varnostni List PDFIljuha9Nessuna valutazione finora
- Daftar Obat Slow Moving Dan Ed Rawat Inap Maret 2021Documento8 pagineDaftar Obat Slow Moving Dan Ed Rawat Inap Maret 2021Vima LadipaNessuna valutazione finora
- Anvisa National Health Surveillance AgencyDocumento52 pagineAnvisa National Health Surveillance AgencyVimarsha HSNessuna valutazione finora
- CCMP 2020 Batch Cardiovascular MCQsDocumento2 pagineCCMP 2020 Batch Cardiovascular MCQsharshad patelNessuna valutazione finora
- Pharmacokinetics and Pharmacodynamics of DrugsDocumento11 paginePharmacokinetics and Pharmacodynamics of Drugsahmalh01Nessuna valutazione finora