Potrebbero piacerti anche
- Pediatric TraumaDocumento446 paginePediatric TraumaMarcec Tea Raveena83% (6)
- Gametogenesis: Spermatogenesis & Oogenesis: Dr. Naveen Kumar MMMC ManipalDocumento16 pagineGametogenesis: Spermatogenesis & Oogenesis: Dr. Naveen Kumar MMMC ManipalLim Yi QiNessuna valutazione finora
- 1F ImmunologyDocumento8 pagine1F ImmunologyDANAH MARGARET VILLAGONZALONessuna valutazione finora
- Accurate Diagnosis of Parasitic Infections Is Important To Decrease The Prevalence andDocumento4 pagineAccurate Diagnosis of Parasitic Infections Is Important To Decrease The Prevalence andManulat VicaiiNessuna valutazione finora
- Guide To History TakingDocumento55 pagineGuide To History TakingGabriella Hild100% (1)
- Head To Toe AssessementDocumento97 pagineHead To Toe AssessementHenry CalisuraNessuna valutazione finora
- Systemic Surgery NuggetsDocumento17 pagineSystemic Surgery NuggetsAhmad UsmanNessuna valutazione finora
- 1 Terminology II LectureDocumento45 pagine1 Terminology II Lecturemaramaliii37Nessuna valutazione finora
- History Taking: DR Anwar H. SiddiquiDocumento26 pagineHistory Taking: DR Anwar H. SiddiquiAssad mustafNessuna valutazione finora
- 4 - Cleavage and BlastulationDocumento31 pagine4 - Cleavage and BlastulationIRENE SEBASTIANNessuna valutazione finora
- Supporting FauciDocumento15 pagineSupporting FauciKelli R. GrantNessuna valutazione finora
- AssessmentDocumento65 pagineAssessmentRitaNessuna valutazione finora
- Decision Making Pain Ramamurthy PDFDocumento319 pagineDecision Making Pain Ramamurthy PDFDian wNessuna valutazione finora
- Development of Gastrointestinal TractDocumento28 pagineDevelopment of Gastrointestinal TractSaif100% (1)
- Examination of Head and Neck SwellingsDocumento22 pagineExamination of Head and Neck SwellingsObehi EromoseleNessuna valutazione finora
- Embryology and Anatomy of The Gastrointestinal TractDocumento58 pagineEmbryology and Anatomy of The Gastrointestinal TractYitancloudNessuna valutazione finora
- Cleavage: The Main Process of Animal DevelopmentDocumento123 pagineCleavage: The Main Process of Animal DevelopmentNUR ASMA RIZKYNessuna valutazione finora
- Medical Terminology-1 2Documento16 pagineMedical Terminology-1 2anneNessuna valutazione finora
- Microbiology MCQ QuestionsDocumento4 pagineMicrobiology MCQ QuestionsNWH Adams LabNessuna valutazione finora
- Problem-based Approach to Gastroenterology and HepatologyDa EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNessuna valutazione finora
- Approach in Lymphadenopathy in ChildrenDocumento14 pagineApproach in Lymphadenopathy in Childrennahiry100% (1)
- 7 Abdominal TraumaDocumento9 pagine7 Abdominal TraumaMyrtle Yvonne RagubNessuna valutazione finora
- Disorders of The Reproductive SystemDocumento10 pagineDisorders of The Reproductive SystemRose Kathreen Quintans AuxteroNessuna valutazione finora
- 3rd Lecture Morphological Changes During Maturation o Te GameteaDocumento25 pagine3rd Lecture Morphological Changes During Maturation o Te GameteaHussein Al Saedi100% (1)
- TrematodesDocumento30 pagineTrematodesJezzah Mae CañeteNessuna valutazione finora
- GROSS ANATOMY-Review Notes PDFDocumento56 pagineGROSS ANATOMY-Review Notes PDFgreen_archerNessuna valutazione finora
- Fall Prevention BrochureDocumento7 pagineFall Prevention Brochurepriyarajan007Nessuna valutazione finora
- eMRCS Pathology 326 MCQsDocumento101 pagineeMRCS Pathology 326 MCQsSaad KhanNessuna valutazione finora
- Mycrobiology ExamDocumento36 pagineMycrobiology ExamSellma Belciler0% (1)
- Myiasis and Strike: Dr. Thahsin Farjana Associate Professor Dept. of Parasitology BAUDocumento33 pagineMyiasis and Strike: Dr. Thahsin Farjana Associate Professor Dept. of Parasitology BAUChuramoni Saha100% (1)
- Community Medicine ItemsDocumento10 pagineCommunity Medicine ItemsMohamed AlaaNessuna valutazione finora
- Pontico en EDocumento16 paginePontico en EKarina OjedaNessuna valutazione finora
- CV - Dr. Atif Ashraf (Physician)Documento6 pagineCV - Dr. Atif Ashraf (Physician)dratifashrafNessuna valutazione finora
- 2023 Introduction To Physical DiagnosisDocumento37 pagine2023 Introduction To Physical DiagnosisNejibMohe Abagisa100% (1)
- GMC M 2022Documento14 pagineGMC M 2022annie000111222333Nessuna valutazione finora
- Membership of The Royal College of PhysiciansDocumento3 pagineMembership of The Royal College of PhysiciansMatin Ahmad KhanNessuna valutazione finora
- Immunobiology Class 8Documento24 pagineImmunobiology Class 8viswas andrewsNessuna valutazione finora
- Grand Rounds Facial Nerve ParalysisDocumento86 pagineGrand Rounds Facial Nerve ParalysisA170riNessuna valutazione finora
- Genetic Counseling and Prenatal DiagnosisDocumento13 pagineGenetic Counseling and Prenatal DiagnosisPande Indra Premana100% (1)
- test1 محولDocumento85 paginetest1 محولTojan Faisal Alzoubi100% (1)
- Test From EmbryologyDocumento25 pagineTest From EmbryologyTreasure ChinenyeNessuna valutazione finora
- Intra Abdominal 2009Documento8 pagineIntra Abdominal 2009Shinta Dwi Septiani Putri WibowoNessuna valutazione finora
- Taking History in PaediatricsDocumento7 pagineTaking History in PaediatricsNikola IgnjatovicNessuna valutazione finora
- Disorder of Sex DevelopmentDocumento40 pagineDisorder of Sex DevelopmentAndi AdityaNessuna valutazione finora
- Answer of Infection and Immunology Mock Exam 9Documento7 pagineAnswer of Infection and Immunology Mock Exam 9Mateen ShukriNessuna valutazione finora
- Early Development in BirdsDocumento53 pagineEarly Development in BirdsMuqaddas NadeemNessuna valutazione finora
- R. Gundo Medical/Surgical Nursing Department: History TakingDocumento39 pagineR. Gundo Medical/Surgical Nursing Department: History Takingchifunndo charlesNessuna valutazione finora
- Abdominal AbscessDocumento3 pagineAbdominal AbscessIchalAzNessuna valutazione finora
- History Taking: 1. DemographicsDocumento12 pagineHistory Taking: 1. Demographicsanis jannahNessuna valutazione finora
- Trichuris Trichiura: Lecture By: Maha Gamal AldeinDocumento20 pagineTrichuris Trichiura: Lecture By: Maha Gamal AldeinMohammad DweibNessuna valutazione finora
- Abdominal Trauma: Fatin Amirah KamaruddinDocumento29 pagineAbdominal Trauma: Fatin Amirah Kamaruddinvirz23Nessuna valutazione finora
- Approach To Comatose ChildDocumento63 pagineApproach To Comatose Childdrmindhacker100% (1)
- Trichuriasis: Disease Type: Parasitic Disease Common Name: Causative Agent: Species of Trichuris Disease DiscriptionDocumento9 pagineTrichuriasis: Disease Type: Parasitic Disease Common Name: Causative Agent: Species of Trichuris Disease DiscriptionBrijesh Singh YadavNessuna valutazione finora
- Cestodes/ Tapeworms CharacteristicsDocumento8 pagineCestodes/ Tapeworms CharacteristicsChinissa Ann LanonNessuna valutazione finora
- AmoebaDocumento5 pagineAmoebasarguss14Nessuna valutazione finora
- Connective TissueDocumento7 pagineConnective TissueSheena Pasion100% (1)
- Clinical Examination of The AbdomenDocumento13 pagineClinical Examination of The AbdomenNur Miladiyah100% (1)
- Parasitilogy: IntroductionDocumento3 pagineParasitilogy: IntroductionJo Marchianne Pigar100% (1)
- CESTODESDocumento10 pagineCESTODEScole_danielleNessuna valutazione finora
- Toacs 2Documento215 pagineToacs 2Mobin Ur Rehman Khan100% (1)
- Diseases of The LarynxDocumento28 pagineDiseases of The LarynxDon AkmalNessuna valutazione finora
- Newborn AssessmentDocumento9 pagineNewborn AssessmentSusmita HalderNessuna valutazione finora
- Pediatrics PerpetualDocumento20 paginePediatrics PerpetualHazel Fernandez VillarNessuna valutazione finora
- MCQs On EpidemiologyDocumento2 pagineMCQs On Epidemiologydmahiu100% (1)
- Samplex ADocumento45 pagineSamplex AAizza ZarateNessuna valutazione finora
- Respiratory System 2011Documento99 pagineRespiratory System 2011Izzah Atqa100% (1)
- TrematodesDocumento5 pagineTrematodesdhaineyNessuna valutazione finora
- Notes On AvesDocumento8 pagineNotes On AvesJessica RoseNessuna valutazione finora
- OSPE 4th Yr PathoDocumento144 pagineOSPE 4th Yr PathoMuhammadShahzadNessuna valutazione finora
- Research Surgery and Care of the Research Animal: Surgical Approaches to the Organ SystemsDa EverandResearch Surgery and Care of the Research Animal: Surgical Approaches to the Organ SystemsNessuna valutazione finora
- Study Report DHF and Dengue Fever, Untuk MuatDocumento13 pagineStudy Report DHF and Dengue Fever, Untuk MuatPande Indra PremanaNessuna valutazione finora
- Alimentary Disorders: Learning TaskDocumento1 paginaAlimentary Disorders: Learning TaskPande Indra PremanaNessuna valutazione finora
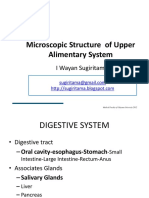
- Upper Alimentary Histology-2012Documento23 pagineUpper Alimentary Histology-2012Pande Indra PremanaNessuna valutazione finora
- Learning Task Alimentary: Self AssessmentDocumento1 paginaLearning Task Alimentary: Self AssessmentPande Indra PremanaNessuna valutazione finora
- Diagnosis Dan Tatalaksana: Nyoman PurwadiDocumento26 pagineDiagnosis Dan Tatalaksana: Nyoman PurwadiPande Indra PremanaNessuna valutazione finora
- New Text DocumentDocumento1 paginaNew Text DocumentPande Indra PremanaNessuna valutazione finora
- Upper Alimentary Histology-2012Documento23 pagineUpper Alimentary Histology-2012Pande Indra PremanaNessuna valutazione finora
- Toxoplasmosis in PregnancyDocumento13 pagineToxoplasmosis in PregnancyPande Indra PremanaNessuna valutazione finora
- 6 ImunoTechniques 2012Documento32 pagine6 ImunoTechniques 2012Pande Indra PremanaNessuna valutazione finora
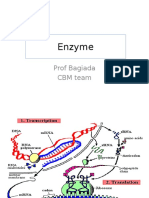
- Enzyme: Prof Bagiada CBM TeamDocumento30 pagineEnzyme: Prof Bagiada CBM TeamPande Indra PremanaNessuna valutazione finora
- Diagnosis and Management of AmebiasisDocumento9 pagineDiagnosis and Management of AmebiasisPande Indra PremanaNessuna valutazione finora
- 2 Organel LinaDocumento34 pagine2 Organel LinaMade WidianantaraNessuna valutazione finora
- 8 Rinitis Alergi Eng VersionDocumento24 pagine8 Rinitis Alergi Eng VersionPande Indra PremanaNessuna valutazione finora
- Uroflowmetry ProcedureDocumento1 paginaUroflowmetry ProcedurePande Indra PremanaNessuna valutazione finora
- Describe of Definition of PolypharmacyDocumento1 paginaDescribe of Definition of PolypharmacyPande Indra PremanaNessuna valutazione finora
- AA Gde Oka Sub-Lab/SMF Urologi FK - UNUD/RSUP Sanglah DenpasarDocumento26 pagineAA Gde Oka Sub-Lab/SMF Urologi FK - UNUD/RSUP Sanglah DenpasarPande Indra PremanaNessuna valutazione finora
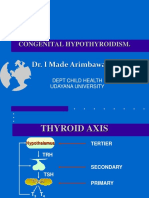
- 19 Congenital HipotiroidDocumento21 pagine19 Congenital HipotiroidPande Indra PremanaNessuna valutazione finora
- 17 Adrenal GlandDocumento33 pagine17 Adrenal GlandPande Indra PremanaNessuna valutazione finora
- Measurements of Morbidity and Mortality in A Population & Source of ErrorDocumento38 pagineMeasurements of Morbidity and Mortality in A Population & Source of ErrorPande Indra PremanaNessuna valutazione finora
- 9 The Balinese TradmedCAMDocumento43 pagine9 The Balinese TradmedCAMPande Indra PremanaNessuna valutazione finora
- Measurements of Morbidity and Mortality in A Population & Source of ErrorDocumento38 pagineMeasurements of Morbidity and Mortality in A Population & Source of ErrorPande Indra PremanaNessuna valutazione finora
- Treatment of Viral InfectionDocumento33 pagineTreatment of Viral InfectionPande Indra PremanaNessuna valutazione finora
- 2 Total Ergonomic ApproachDocumento25 pagine2 Total Ergonomic ApproachPande Indra PremanaNessuna valutazione finora
- Pathogenesis of Bacterial Infection Sem 3Documento46 paginePathogenesis of Bacterial Infection Sem 3Sheryl ElitaNessuna valutazione finora
- 19 Congenital HipotiroidDocumento21 pagine19 Congenital HipotiroidPande Indra PremanaNessuna valutazione finora
- Rheumatoid Arthrirtis & Systemic Lupus Erythematosus: Interactive Lecture of Clinical Immune DisorderDocumento53 pagineRheumatoid Arthrirtis & Systemic Lupus Erythematosus: Interactive Lecture of Clinical Immune DisorderPande Indra PremanaNessuna valutazione finora
- Achondroplasia Emedicine DKKDocumento29 pagineAchondroplasia Emedicine DKKPande Indra PremanaNessuna valutazione finora
- Nama: Pande Ketut Astri Utami No: 33 Kelas: Vii GDocumento3 pagineNama: Pande Ketut Astri Utami No: 33 Kelas: Vii GPande Indra PremanaNessuna valutazione finora
- Pediatric Assessment TriangleDocumento13 paginePediatric Assessment TriangleShinta NareswariNessuna valutazione finora
- Telaah JurnalDocumento29 pagineTelaah JurnalRafiqy Sa'adiy FaizunNessuna valutazione finora
- PATIENT MONITOR SpesifikasiDocumento3 paginePATIENT MONITOR SpesifikasiAmanda DavisNessuna valutazione finora
- FINAL Use and Application of Topical FluoridesDocumento7 pagineFINAL Use and Application of Topical FluoridesmahmoudNessuna valutazione finora
- Dentj 39 3 04Documento10 pagineDentj 39 3 04Ngakan OkaNessuna valutazione finora
- Soft Drinks and Dental Health A Review PDFDocumento10 pagineSoft Drinks and Dental Health A Review PDFMarcelaNessuna valutazione finora
- Canadanian Jurnal Diabetes PDFDocumento342 pagineCanadanian Jurnal Diabetes PDFdyahNessuna valutazione finora
- Ventilator Associated Pneumonia in ChildrenDocumento7 pagineVentilator Associated Pneumonia in ChildrendarlingcarvajalduqueNessuna valutazione finora
- 1.7 Surgery For Cyst or Abscess of The Bartholin Gland With Special Reference To The Newer OperatasDocumento3 pagine1.7 Surgery For Cyst or Abscess of The Bartholin Gland With Special Reference To The Newer OperatasMuh IkhsanNessuna valutazione finora
- Newborn Discharge Instruction 2015Documento4 pagineNewborn Discharge Instruction 2015Carla AbalaNessuna valutazione finora
- Nitrous Oxide Diffusion and The Second Gas Effect.26Documento7 pagineNitrous Oxide Diffusion and The Second Gas Effect.26Syukron AmrullahNessuna valutazione finora
- Spinal Implants - Interplate C-PDocumento5 pagineSpinal Implants - Interplate C-PperfectspineNessuna valutazione finora
- HPCZ Application FormDocumento11 pagineHPCZ Application FormQualis LabsNessuna valutazione finora
- 1 The Philippines Sam Guidelines 2015 Final Print Ready PDFDocumento111 pagine1 The Philippines Sam Guidelines 2015 Final Print Ready PDFFar SultanNessuna valutazione finora
- GastroenteritisDocumento24 pagineGastroenteritisMomogi ForeverhappyNessuna valutazione finora
- OkokosDocumento3 pagineOkokoskaulauNessuna valutazione finora
- Jackie Zema Dietitian ResumeDocumento2 pagineJackie Zema Dietitian Resumeapi-359505576Nessuna valutazione finora
- Physician CatalogDocumento573 paginePhysician CatalogIfan RizkyNessuna valutazione finora
- The Function and Importance of Incisal Guidance inDocumento75 pagineThe Function and Importance of Incisal Guidance inPragya Jain100% (1)
- Manual de Especialidades Medicas en InglesDocumento117 pagineManual de Especialidades Medicas en InglesYobelkisNessuna valutazione finora
- Makalah Bahasa InggrisDocumento11 pagineMakalah Bahasa Inggrismei diana sara'isNessuna valutazione finora