Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Ultrasound Spectrum in Intraductal Papillary Neoplasms of BreastDocumento7 pagineUltrasound Spectrum in Intraductal Papillary Neoplasms of BreastdrrahulsshindeNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Tubeless Hypotonic DuodenographyDocumento12 pagineTubeless Hypotonic DuodenographydrrahulsshindeNessuna valutazione finora
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- Surgical Anatomy PF PNSDocumento11 pagineSurgical Anatomy PF PNSdrrahulsshindeNessuna valutazione finora
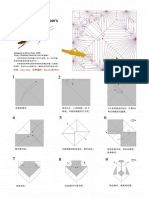
- Brian Chan-Locust PDFDocumento10 pagineBrian Chan-Locust PDFdrrahulsshindeNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Frontal Sinus Drainage Pathway PDFDocumento9 pagineFrontal Sinus Drainage Pathway PDFdrrahulsshindeNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Quarterly Oru Folding Diagrams - Vol.2Documento186 pagineQuarterly Oru Folding Diagrams - Vol.2drrahulsshinde89% (19)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Quarterly Oru Folding Diagrams Vol 1Documento199 pagineQuarterly Oru Folding Diagrams Vol 1drrahulsshinde95% (20)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Adult Obesity ResearchDocumento19 pagineAdult Obesity Researchchoraz100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Residents Self Assessment FormDocumento5 pagineResidents Self Assessment Formapi-245673459Nessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Neurological Reorganization For Brain Injury by Sargent L. Goodchild, Jr.Documento6 pagineNeurological Reorganization For Brain Injury by Sargent L. Goodchild, Jr.autismoneNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Maria Encarnacion RESUMEDocumento2 pagineMaria Encarnacion RESUMEarlyn encarnacionNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Developing Geriatric Services For Incontinence in The ElderlyDocumento5 pagineDeveloping Geriatric Services For Incontinence in The ElderlyrnrmmanphdNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- BioginkgoDocumento8 pagineBioginkgoCherry San DiegoNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Running Head: Mass Incarceration and Politics 1Documento16 pagineRunning Head: Mass Incarceration and Politics 1kimoda freelancerNessuna valutazione finora
- Anatomy and PhysiologyDocumento8 pagineAnatomy and PhysiologyteGraWN100% (1)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Russian Current Shiva Sarari 1Documento25 pagineRussian Current Shiva Sarari 1Sharma MukeshNessuna valutazione finora
- Bajaj Committee Report 1996Documento267 pagineBajaj Committee Report 1996lalit823187Nessuna valutazione finora
- Nerc Annual Essay CompetitionDocumento2 pagineNerc Annual Essay CompetitionFalade LadsNessuna valutazione finora
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- Danica Hannah Mae L. Tumacder Bsed 2B MWF 4-5PM Assignment: Ge Sts APRIL 12, 2021Documento4 pagineDanica Hannah Mae L. Tumacder Bsed 2B MWF 4-5PM Assignment: Ge Sts APRIL 12, 2021Nica HannahNessuna valutazione finora
- AMLDocumento19 pagineAMLquerokeropi100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- Dental Negligence in Clinical PracticeDocumento18 pagineDental Negligence in Clinical PracticeLutfun NessaNessuna valutazione finora
- Peace Corps MS 261 Policy 2017 - BackUp Medical ProviderDocumento8 paginePeace Corps MS 261 Policy 2017 - BackUp Medical ProviderAccessible Journal Media: Peace Corps DocumentsNessuna valutazione finora
- Disaster Management Continuum Pre-DisasterDocumento2 pagineDisaster Management Continuum Pre-DisasterPearl JuntillaNessuna valutazione finora
- Daily Instructional Lesson Plan: Worcester County Public SchoolsDocumento6 pagineDaily Instructional Lesson Plan: Worcester County Public Schoolsapi-309747527Nessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Stimulus Piece PTSD AnswersDocumento2 pagineStimulus Piece PTSD AnswerschandanaNessuna valutazione finora
- RPH 2Documento3 pagineRPH 2AYEN AROBINTONessuna valutazione finora
- Clinical Optometry Primary Eye CareDocumento3 pagineClinical Optometry Primary Eye CareDanielle SangalangNessuna valutazione finora
- NEW Periodontal ClassificationDocumento7 pagineNEW Periodontal ClassificationCarlos MikaelNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Swine Infectious Gastrointestinal DiseasesDocumento6 pagineSwine Infectious Gastrointestinal DiseasesnessimmounirNessuna valutazione finora
- Коспект лекційDocumento51 pagineКоспект лекційМарія МайорчакNessuna valutazione finora
- TAYLOR 1984 AnaesthesiaDocumento3 pagineTAYLOR 1984 Anaesthesiapolly91Nessuna valutazione finora
- 3202 7164 1 SMDocumento21 pagine3202 7164 1 SMPetrus Yendi SaputraNessuna valutazione finora
- Geriatric Index of Comorbidity: Validation and Comparison With Other Measures of ComorbidityDocumento9 pagineGeriatric Index of Comorbidity: Validation and Comparison With Other Measures of ComorbidityDesya EspriliaNessuna valutazione finora
- Predicting Physiological Capacity of Human Load Carriage - A ReviewDocumento10 paginePredicting Physiological Capacity of Human Load Carriage - A ReviewlnarimotoNessuna valutazione finora
- English For Nurses-Vital Signs and MonitoringDocumento5 pagineEnglish For Nurses-Vital Signs and MonitoringSorana PaleuNessuna valutazione finora
- Australian Indigenous People - EditedDocumento8 pagineAustralian Indigenous People - EditedApril CliffordNessuna valutazione finora
- Bloodborne Pathogen Training PDFDocumento22 pagineBloodborne Pathogen Training PDFapi-282330630Nessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)