Potrebbero piacerti anche
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- The Electricity Act - 2003Documento84 pagineThe Electricity Act - 2003Anshul PandeyNessuna valutazione finora
- Newsletter 289Documento10 pagineNewsletter 289Henry CitizenNessuna valutazione finora
- Portrait of An INTJDocumento2 paginePortrait of An INTJDelia VlasceanuNessuna valutazione finora
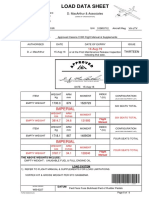
- Load Data Sheet: ImperialDocumento3 pagineLoad Data Sheet: ImperialLaurean Cub BlankNessuna valutazione finora
- Efs151 Parts ManualDocumento78 pagineEfs151 Parts ManualRafael VanegasNessuna valutazione finora
- 1 PBDocumento14 pagine1 PBSaepul HayatNessuna valutazione finora
- 90FF1DC58987 PDFDocumento9 pagine90FF1DC58987 PDFfanta tasfayeNessuna valutazione finora
- Astm E53 98Documento1 paginaAstm E53 98park991018Nessuna valutazione finora
- MSDS - Tuff-Krete HD - Part DDocumento6 pagineMSDS - Tuff-Krete HD - Part DAl GuinitaranNessuna valutazione finora
- TLE - IA - Carpentry Grades 7-10 CG 04.06.2014Documento14 pagineTLE - IA - Carpentry Grades 7-10 CG 04.06.2014RickyJeciel100% (2)
- DesalinationDocumento4 pagineDesalinationsivasu1980aNessuna valutazione finora
- CNC USB English ManualDocumento31 pagineCNC USB English ManualHarold Hernan MuñozNessuna valutazione finora
- Brochure Ref 670Documento4 pagineBrochure Ref 670veerabossNessuna valutazione finora
- 4 Bar LinkDocumento4 pagine4 Bar LinkConstance Lynn'da GNessuna valutazione finora
- How Yaffs WorksDocumento25 pagineHow Yaffs WorkseemkutayNessuna valutazione finora
- Fidp ResearchDocumento3 pagineFidp ResearchIn SanityNessuna valutazione finora
- Innovations in Land AdministrationDocumento66 pagineInnovations in Land AdministrationSanjawe KbNessuna valutazione finora
- Google App EngineDocumento5 pagineGoogle App EngineDinesh MudirajNessuna valutazione finora
- Agfa CR 85-X: Specification Fuji FCR Xg5000 Kodak CR 975Documento3 pagineAgfa CR 85-X: Specification Fuji FCR Xg5000 Kodak CR 975Youness Ben TibariNessuna valutazione finora
- TAB Procedures From An Engineering FirmDocumento18 pagineTAB Procedures From An Engineering Firmtestuser180Nessuna valutazione finora
- Reflections On Free MarketDocumento394 pagineReflections On Free MarketGRK MurtyNessuna valutazione finora
- Oracle FND User APIsDocumento4 pagineOracle FND User APIsBick KyyNessuna valutazione finora
- Expense Tracking - How Do I Spend My MoneyDocumento2 pagineExpense Tracking - How Do I Spend My MoneyRenata SánchezNessuna valutazione finora
- Strobostomp HD™ Owner'S Instruction Manual V1.1 En: 9V DC Regulated 85maDocumento2 pagineStrobostomp HD™ Owner'S Instruction Manual V1.1 En: 9V DC Regulated 85maShane FairchildNessuna valutazione finora
- 450i User ManualDocumento54 pagine450i User ManualThượng Lê Văn0% (2)
- Apm p5 Course NotesDocumento267 pagineApm p5 Course NotesMusumbulwe Sue MambweNessuna valutazione finora
- Introduce Letter - CV IDS (Company Profile)Documento13 pagineIntroduce Letter - CV IDS (Company Profile)katnissNessuna valutazione finora
- Tivoli Performance ViewerDocumento4 pagineTivoli Performance ViewernaveedshakurNessuna valutazione finora
- CANELA Learning Activity - NSPE Code of EthicsDocumento4 pagineCANELA Learning Activity - NSPE Code of EthicsChristian CanelaNessuna valutazione finora
- EXTENDED PROJECT-Shoe - SalesDocumento28 pagineEXTENDED PROJECT-Shoe - Salesrhea100% (5)