Potrebbero piacerti anche
- Delivery of TwinsDocumento25 pagineDelivery of TwinsCakraEkkyNessuna valutazione finora
- Uncontrolled Blood Sugar NCPDocumento4 pagineUncontrolled Blood Sugar NCPRawan KhateebNessuna valutazione finora
- Thyroid Cancer: Causes, Types, Diagnosis and TreatmentDocumento38 pagineThyroid Cancer: Causes, Types, Diagnosis and TreatmentsarahNessuna valutazione finora
- Graves' Hyperthyroidism in Pregnancy: A Clinical ReviewDocumento22 pagineGraves' Hyperthyroidism in Pregnancy: A Clinical ReviewAnisa Dinda NurlianaNessuna valutazione finora
- Abnormal Thyroid Function in PregnancyDocumento54 pagineAbnormal Thyroid Function in Pregnancyasri khazaliNessuna valutazione finora
- Hypothyroidism in PregnancyDocumento14 pagineHypothyroidism in PregnancyShajia ZafarNessuna valutazione finora
- Hypothyroid in Pregnancy Andi CakraDocumento32 pagineHypothyroid in Pregnancy Andi CakraCakraEkkyNessuna valutazione finora
- Thyroid DX PXLDocumento62 pagineThyroid DX PXLabduljebarNessuna valutazione finora
- Hyperthyroidsm: EpidemiologyDocumento6 pagineHyperthyroidsm: EpidemiologyEllieNessuna valutazione finora
- Hypothyroidism in Pregnancy: Causes, Effects and ManagementDocumento29 pagineHypothyroidism in Pregnancy: Causes, Effects and ManagementhanaddulNessuna valutazione finora
- Thyroid Function TestDocumento28 pagineThyroid Function TestDhinesh Muthusamy100% (1)
- Guidelines of The American Thyroid Association PREGNANCY PDFDocumento47 pagineGuidelines of The American Thyroid Association PREGNANCY PDFIqra AnugerahNessuna valutazione finora
- Thyroid and InfertilityDocumento36 pagineThyroid and InfertilitySairindri SahooNessuna valutazione finora
- The Role of Maternal Thyroid Status On Pregnancy Outcome For Motherand NewbornDocumento36 pagineThe Role of Maternal Thyroid Status On Pregnancy Outcome For Motherand NewbornRahmayantiYuliaNessuna valutazione finora
- Levothyroxine in TPO+ euthyroid women before conceptionDocumento18 pagineLevothyroxine in TPO+ euthyroid women before conceptionRoxana TudorNessuna valutazione finora
- Biol 460 Case StudyDocumento11 pagineBiol 460 Case Studyapi-353888678Nessuna valutazione finora
- Thyroid DisordersDocumento29 pagineThyroid DisordersEMPINessuna valutazione finora
- Gds137 Slide HyperthyroidismDocumento30 pagineGds137 Slide HyperthyroidismLouie Kem Anthony BabaranNessuna valutazione finora
- Week 3 Pharmaco Part 2Documento34 pagineWeek 3 Pharmaco Part 2Tiko JomidavaNessuna valutazione finora
- Let's Talk About Thyroid PDFDocumento92 pagineLet's Talk About Thyroid PDFEidi IdhamNessuna valutazione finora
- Endocrine 160110083024Documento65 pagineEndocrine 160110083024Ryan CracknellNessuna valutazione finora
- Thyroid Panel-1 (T3/T4/TSH) : Investigation Observed Value Unit Biological Reference IntervalDocumento2 pagineThyroid Panel-1 (T3/T4/TSH) : Investigation Observed Value Unit Biological Reference IntervalShashikantNessuna valutazione finora
- Thyroid Emergencies-Dr. AM IyagbaDocumento13 pagineThyroid Emergencies-Dr. AM IyagbaDr. Amb. Monday ZaccheausNessuna valutazione finora
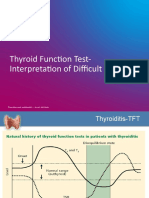
- TFT Interpretation of Difficult CasesDocumento51 pagineTFT Interpretation of Difficult CasesAditya GautamNessuna valutazione finora
- Obsgin - Dr. Dr. Freddy W. Wagey, SpOG-KDocumento26 pagineObsgin - Dr. Dr. Freddy W. Wagey, SpOG-KDedy SupriadiNessuna valutazione finora
- Hyperthyroidism: A Practical Approach To Diagnosis and ManagementDocumento70 pagineHyperthyroidism: A Practical Approach To Diagnosis and ManagementMutiara Manuella TambaNessuna valutazione finora
- Preeclampsia Liver DysfunctionDocumento5 paginePreeclampsia Liver DysfunctionDesyHandayaniNessuna valutazione finora
- Conference Brochure With Link7Documento16 pagineConference Brochure With Link7Shrutik AshiyaniNessuna valutazione finora
- Recurrent Pregnancy LossDocumento19 pagineRecurrent Pregnancy LossSean NamNessuna valutazione finora
- Lesi PrakankerDocumento60 pagineLesi PrakankerObgynism 2019Nessuna valutazione finora
- AACE and ATA 2012 Clinical Practice Guidelines for HypothyroidismDocumento63 pagineAACE and ATA 2012 Clinical Practice Guidelines for HypothyroidismNur Rakhma AkmaliaNessuna valutazione finora
- AmenorrheaDocumento56 pagineAmenorrheaMrTriumphantNessuna valutazione finora
- Sirkulasi UteroplasentaDocumento16 pagineSirkulasi UteroplasentaPriscilla BudhipramonoNessuna valutazione finora
- Hypertensive Disorder in Pregnancy Untuk KuliahDocumento78 pagineHypertensive Disorder in Pregnancy Untuk Kuliah404notfoundNessuna valutazione finora
- Variations, Errors, and QualityDocumento46 pagineVariations, Errors, and QualityJohn Reden RomeroNessuna valutazione finora
- Obat antithiroid: New England Medical Journal review of antithyroid drugsDocumento52 pagineObat antithiroid: New England Medical Journal review of antithyroid drugsYeyen MusainiNessuna valutazione finora
- Abnormal Uterine Bleeding: District 1 ACOG Medical Student Education Module 2008Documento17 pagineAbnormal Uterine Bleeding: District 1 ACOG Medical Student Education Module 2008ninachayank0% (1)
- FunctionTests Brochure PDFDocumento2 pagineFunctionTests Brochure PDFArslan SaleemNessuna valutazione finora
- CHN1 Health Care Delivery System2Documento22 pagineCHN1 Health Care Delivery System2MicaNessuna valutazione finora
- Seminar 5 - Thyroid Disease in PregnancyDocumento25 pagineSeminar 5 - Thyroid Disease in PregnancyHakimah K. SuhaimiNessuna valutazione finora
- Placental PathologyDocumento465 paginePlacental PathologyOana Roxana PuscasNessuna valutazione finora
- Understanding Miscarriage: Causes, Symptoms and TreatmentDocumento33 pagineUnderstanding Miscarriage: Causes, Symptoms and TreatmentIsmail FaruqiNessuna valutazione finora
- Gestational Trophoblastic Disease Pt2Documento75 pagineGestational Trophoblastic Disease Pt2yurie_ameliaNessuna valutazione finora
- Early Pregnancy LossDocumento20 pagineEarly Pregnancy LossRima HajjarNessuna valutazione finora
- Simposium 1 - Controversies - Dr. Teguh - HPV Vaccine Vs HPV Test-1Documento20 pagineSimposium 1 - Controversies - Dr. Teguh - HPV Vaccine Vs HPV Test-1isnayu drNessuna valutazione finora
- CBD Hiperemis GravidarumDocumento32 pagineCBD Hiperemis GravidarumFifit SiePutry BintaNgnya KudaciNessuna valutazione finora
- Graves' Disease & PregnancyDocumento19 pagineGraves' Disease & Pregnancyrajan kumar100% (1)
- Abortion PresentationDocumento46 pagineAbortion PresentationJhong Xyrus67% (3)
- Implantation and Development Placenta Part 2Documento36 pagineImplantation and Development Placenta Part 2Tengku Chairannisa PutriNessuna valutazione finora
- Interna Medicine Case Report Prof. Dr. W. Z. Johannes Hospital AUGUST 2019 Medical Faculty Nusa Cendana UniversityDocumento46 pagineInterna Medicine Case Report Prof. Dr. W. Z. Johannes Hospital AUGUST 2019 Medical Faculty Nusa Cendana UniversityErni JawaNessuna valutazione finora
- Interpreting Thyroid Tests: Key FactorsDocumento7 pagineInterpreting Thyroid Tests: Key FactorsStrawberry ShortcakeNessuna valutazione finora
- Polycystic Ovarian Syndrome (PCOS)Documento57 paginePolycystic Ovarian Syndrome (PCOS)Michelle FynesNessuna valutazione finora
- '3'hyperthyroid and HypothyroidDocumento42 pagine'3'hyperthyroid and Hypothyroidafriskha bulawanNessuna valutazione finora
- Janica E. Walden, MD Neuroradiology University of North CarolinaDocumento21 pagineJanica E. Walden, MD Neuroradiology University of North CarolinaBilly ChietraNessuna valutazione finora
- Overview Antenatal CareDocumento54 pagineOverview Antenatal CareRizky Dwidya AmirtasariNessuna valutazione finora
- Surgical Pathology For Dentistry Students - Surgical Pathology of Thyroid and Adrenal GlandsDocumento38 pagineSurgical Pathology For Dentistry Students - Surgical Pathology of Thyroid and Adrenal Glandssorin niky mocanu100% (1)
- KB HormonalDocumento65 pagineKB Hormonaljessica_siahaan_1Nessuna valutazione finora
- Anemia Prenatal Care - DR - Rima IrwindaDocumento43 pagineAnemia Prenatal Care - DR - Rima IrwindaHari SandiNessuna valutazione finora
- Gestational Trophoblastic DiseasesDocumento37 pagineGestational Trophoblastic DiseasesEdwin OkonNessuna valutazione finora
- REFERAT - Ppt.solusio Plasenta ItaDocumento18 pagineREFERAT - Ppt.solusio Plasenta ItaMochammad Adam EldiNessuna valutazione finora
- Lesi Prakanker & Tumor Ginekologi (Versi 2003)Documento71 pagineLesi Prakanker & Tumor Ginekologi (Versi 2003)Satwika EkanandaNessuna valutazione finora
- Bab IDocumento36 pagineBab IDiga AnaNessuna valutazione finora
- Thyroid Disorders During PregnancyDocumento25 pagineThyroid Disorders During PregnancyA.H.ANessuna valutazione finora
- AnemiaDocumento29 pagineAnemiaCakraEkkyNessuna valutazione finora
- HipothyroidDocumento48 pagineHipothyroidCakraEkkyNessuna valutazione finora
- 27Documento55 pagine27kutra3000Nessuna valutazione finora
- Seleneum in ReproductiveDocumento19 pagineSeleneum in ReproductiveCakraEkkyNessuna valutazione finora
- Seleneum in ReproductiveDocumento19 pagineSeleneum in ReproductiveCakraEkkyNessuna valutazione finora
- Pemeriksaan Laboratorium Hormon Tiroid: Oleh: Dr. Diah Hermayanti, SPPKDocumento16 paginePemeriksaan Laboratorium Hormon Tiroid: Oleh: Dr. Diah Hermayanti, SPPKZulfan RifqiawanNessuna valutazione finora
- School nurse develops diabetic planDocumento2 pagineSchool nurse develops diabetic plantycheNessuna valutazione finora
- 72 Endo AnnotatedDocumento9 pagine72 Endo AnnotatedErika ArceoNessuna valutazione finora
- Preventing Diabetes in Pregnant WomenDocumento5 paginePreventing Diabetes in Pregnant WomenJulina Br SembiringNessuna valutazione finora
- Kurnia Minanur Rokhman Nim. A01502079Documento71 pagineKurnia Minanur Rokhman Nim. A01502079sri ganti pangaribuanNessuna valutazione finora
- EBM - Diabetes Guidelines (Javidan) 7Documento198 pagineEBM - Diabetes Guidelines (Javidan) 7Ash JavidanNessuna valutazione finora
- DisfungsiDocumento1 paginaDisfungsiHandayan HtbNessuna valutazione finora
- Study of Histopathological Pattern of Thyroid Lesions: International Journal of Biomedical and Advance ResearchDocumento10 pagineStudy of Histopathological Pattern of Thyroid Lesions: International Journal of Biomedical and Advance ResearchAprilia Fani PNessuna valutazione finora
- 8 PathoDocumento2 pagine8 PathoKris LingadNessuna valutazione finora
- Referat 6. Daftar Pustaka HipertiroidDocumento2 pagineReferat 6. Daftar Pustaka HipertiroidSigit Dwi RahardjoNessuna valutazione finora
- MCQs ThyroidtDocumento14 pagineMCQs ThyroidtAhmed Attia100% (5)
- Fasting Plasma Glucose: Test Report Mr. Sambasiva 51 Years / MaleDocumento5 pagineFasting Plasma Glucose: Test Report Mr. Sambasiva 51 Years / Malemathesis-2Nessuna valutazione finora
- Skripsi Tanpa Bab PembahasanDocumento65 pagineSkripsi Tanpa Bab PembahasanTondi Rosalinda SinagaNessuna valutazione finora
- Workbook - 4 CDocumento51 pagineWorkbook - 4 CDebbieNessuna valutazione finora
- Summary of Antidiabetic Drugs PDFDocumento3 pagineSummary of Antidiabetic Drugs PDFZinc YuloNessuna valutazione finora
- Effect of Diet On Type 2 Diabetes MellitusDocumento14 pagineEffect of Diet On Type 2 Diabetes MellitusPriya bhattiNessuna valutazione finora
- HbA1c (Glycosylated HB)Documento3 pagineHbA1c (Glycosylated HB)يوسف الشرقاويNessuna valutazione finora
- HyperthyroidismDocumento59 pagineHyperthyroidismSehrish Khan100% (1)
- Daily Patterns: 6.6% or 49 Mmol/molDocumento6 pagineDaily Patterns: 6.6% or 49 Mmol/molD V BHASKARNessuna valutazione finora
- Malignant Thyroid and Parathyroid DisordersDocumento48 pagineMalignant Thyroid and Parathyroid DisordersPavan chowdaryNessuna valutazione finora
- DIABETES MELLITUS SIGNS AND SYMPTOMSDocumento3 pagineDIABETES MELLITUS SIGNS AND SYMPTOMSMutiara yunitaNessuna valutazione finora
- Global Epidemiology of Hyperthyroidism and Hypothyroidism: Nature Reviews Endocrinology March 2018Documento17 pagineGlobal Epidemiology of Hyperthyroidism and Hypothyroidism: Nature Reviews Endocrinology March 2018yenny handayani sihiteNessuna valutazione finora
- Kegawatdaruratan Diabetes Melitus: Terapi Insulin IntravenaDocumento27 pagineKegawatdaruratan Diabetes Melitus: Terapi Insulin IntravenaSesilia Sri Yanti GaddyNessuna valutazione finora
- Group 1 TCM Assigment 1Documento4 pagineGroup 1 TCM Assigment 1mayaNessuna valutazione finora
- Bomba MedtronicDocumento40 pagineBomba MedtronicrafaelplNessuna valutazione finora
- Dexamethasone Suppression TestDocumento2 pagineDexamethasone Suppression Testjbeans92Nessuna valutazione finora
- Thyroid DisorderDocumento20 pagineThyroid DisorderNadun MethwadaneNessuna valutazione finora
- GDMDocumento12 pagineGDMJennicaNessuna valutazione finora