Potrebbero piacerti anche
- SinulDocumento86 pagineSinulCucos NataliaNessuna valutazione finora
- Anatomy of The Pectoral RegionDocumento42 pagineAnatomy of The Pectoral Regionomotayojane21Nessuna valutazione finora
- Anatomy Screeningcervix by DR. VACHASPATIDocumento52 pagineAnatomy Screeningcervix by DR. VACHASPATIOshydh PojnNessuna valutazione finora
- Anatomy of The UterusDocumento21 pagineAnatomy of The UterusSalman KhanNessuna valutazione finora
- P. Cavity: (Female Reproductive Organs)Documento38 pagineP. Cavity: (Female Reproductive Organs)SAKARIYE MAXAMEDNessuna valutazione finora
- Anatomical Considerations During G-Laparoscopic SurgeryDocumento28 pagineAnatomical Considerations During G-Laparoscopic SurgeryMahia RahmanNessuna valutazione finora
- Abdominal Wall and HerniaDocumento35 pagineAbdominal Wall and HerniaMohammad BanisalmanNessuna valutazione finora
- Uterus Fallopian Tube and OvaryDocumento35 pagineUterus Fallopian Tube and Ovaryvijaya pranaviNessuna valutazione finora
- Lec.1.Anatomy of PregnancyDocumento53 pagineLec.1.Anatomy of PregnancyManal AsadNessuna valutazione finora
- Anatomy of GIT For PCII Students..Documento106 pagineAnatomy of GIT For PCII Students..AMANUEL HABTEWOLDNessuna valutazione finora
- Female Genital OrgansDocumento40 pagineFemale Genital OrgansShimmering MoonNessuna valutazione finora
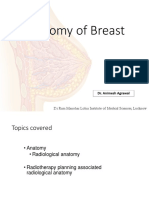
- Anatomy of Breast: DR Ram Manohar Lohia Institute of Medical Sciences, LucknowDocumento103 pagineAnatomy of Breast: DR Ram Manohar Lohia Institute of Medical Sciences, LucknowMohammad Ahmad AyasrahNessuna valutazione finora
- Anatomy of Fallopian Tube & OvaryDocumento89 pagineAnatomy of Fallopian Tube & OvaryAsma AijazNessuna valutazione finora
- Surgical-ANATOMY OF Anterior Abdominal WallDocumento83 pagineSurgical-ANATOMY OF Anterior Abdominal WallSyed Irfan ArifNessuna valutazione finora
- Anatomy of The Breast1Documento13 pagineAnatomy of The Breast1Shahinda Ahmed AdelNessuna valutazione finora
- AnatDocumento45 pagineAnatRinxas VerinxtNessuna valutazione finora
- Breast Anatomy With Clinical CorrelationDocumento27 pagineBreast Anatomy With Clinical CorrelationDionix Cruz100% (2)
- Anatomy and Physiology of The VaginaDocumento74 pagineAnatomy and Physiology of The VaginaRacquel BurrowesNessuna valutazione finora
- Breast AnatomyDocumento15 pagineBreast Anatomyvarun100% (1)
- Anterolateral Abdominal Wall and Abdominal IncisionsDocumento42 pagineAnterolateral Abdominal Wall and Abdominal IncisionsSamar AhmadNessuna valutazione finora
- Abdomen and Abdominal WallDocumento40 pagineAbdomen and Abdominal WallAlex ChagalaNessuna valutazione finora
- Embryology and Functional Anatomy of The BreastDocumento20 pagineEmbryology and Functional Anatomy of The BreastseidkeNessuna valutazione finora
- Abdominal Region Part 2Documento58 pagineAbdominal Region Part 2Swati LataNessuna valutazione finora
- Breast - Mammary GlandDocumento16 pagineBreast - Mammary GlandEniola DaramolaNessuna valutazione finora
- Uterus and Ovary UltrasoundDocumento144 pagineUterus and Ovary Ultrasoundisicheipraise3Nessuna valutazione finora
- Anatomy of Female Reproductive SystemDocumento68 pagineAnatomy of Female Reproductive SystemdodoNessuna valutazione finora
- 4rd Lecture - AbdomenDocumento26 pagine4rd Lecture - AbdomenZainab Jamal SiddiquiNessuna valutazione finora
- Anatomy and Embryology of Bladder: Dr. Deepesh Kalra Institute of Urology Madras Medical College, ChennaiDocumento33 pagineAnatomy and Embryology of Bladder: Dr. Deepesh Kalra Institute of Urology Madras Medical College, ChennaiFatima Zahra Rahim ArchiNessuna valutazione finora
- 4) Mammary Gland 220413 Upnm2Documento22 pagine4) Mammary Gland 220413 Upnm2AaronMaroonFive100% (1)
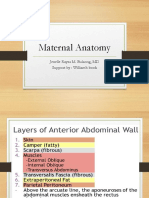
- Maternal Anatomy WilliamsDocumento60 pagineMaternal Anatomy WilliamsZari Novela100% (2)
- Female Genital Organs.Documento18 pagineFemale Genital Organs.Shimmering MoonNessuna valutazione finora
- Topography Femoral RegionDocumento40 pagineTopography Femoral RegionmonaNessuna valutazione finora
- Perineal TearsDocumento49 paginePerineal TearsvisakhaNessuna valutazione finora
- Vagina Anat, Episiotomy and MGMT of Cervical TearDocumento50 pagineVagina Anat, Episiotomy and MGMT of Cervical TearCapricious BibekNessuna valutazione finora
- Intro Lab Anatomi Rps (2024)Documento117 pagineIntro Lab Anatomi Rps (2024)Jason Maxwell mcguireNessuna valutazione finora
- Abdominal WallDocumento56 pagineAbdominal WallAHMAD KHANNessuna valutazione finora
- PT Physiology of PuerperiumDocumento14 paginePT Physiology of PuerperiumPragati BholeNessuna valutazione finora
- Revisit of Male & Female Genital Tracts Semester VIIDocumento50 pagineRevisit of Male & Female Genital Tracts Semester VIIDr. AyshaNessuna valutazione finora
- 07 - Uterus, Uterine Tubes, OvariesDocumento52 pagine07 - Uterus, Uterine Tubes, Ovariesck4realNessuna valutazione finora
- AnatomicallyDocumento3 pagineAnatomicallyAjayDeep NallabothulaNessuna valutazione finora
- CBL 2Documento20 pagineCBL 2Hammad AkramNessuna valutazione finora
- Anatomy of Uterus and Vagina and PudendumDocumento38 pagineAnatomy of Uterus and Vagina and Pudendumgugus aminaNessuna valutazione finora
- Female PerineumDocumento27 pagineFemale Perineumkaartikey dubeNessuna valutazione finora
- Anterior Abdominal Wall& Inguinal Canal 2023Documento26 pagineAnterior Abdominal Wall& Inguinal Canal 2023GanapathyGaneshNessuna valutazione finora
- Ca BreastDocumento64 pagineCa Breastadina.batajuNessuna valutazione finora
- Perineum and UG TriangleDocumento27 paginePerineum and UG TriangleAbiola NerdNessuna valutazione finora
- Maternal AnatomyDocumento96 pagineMaternal AnatomyIbnu RahmanNessuna valutazione finora
- UntitledDocumento7 pagineUntitledDania Ibraheem100% (1)
- Student Name: ALI HASSAN RAZA STUDENT I D: 2018304027Documento6 pagineStudent Name: ALI HASSAN RAZA STUDENT I D: 2018304027Sayed AsifNessuna valutazione finora
- Perineum AnatomyDocumento23 paginePerineum Anatomyrohitrohillapalwal999Nessuna valutazione finora
- Anatomy of Pregnancy NewDocumento42 pagineAnatomy of Pregnancy NewZaroon Abdullah KhanNessuna valutazione finora
- Relations of ThoraxDocumento28 pagineRelations of ThoraxAnigha PrasadNessuna valutazione finora
- Anatomy and PhysiologyDocumento3 pagineAnatomy and PhysiologyJade AltarejosNessuna valutazione finora
- Inguinal Canal: DR - Lubna NazliDocumento28 pagineInguinal Canal: DR - Lubna NazliAhmed AminNessuna valutazione finora
- UterusDocumento34 pagineUterushammad992Nessuna valutazione finora
- Urinary Bladder, Rectum and Anal CanalDocumento34 pagineUrinary Bladder, Rectum and Anal CanalIbe ClementNessuna valutazione finora
- Uterus 1Documento13 pagineUterus 1shrutik91Nessuna valutazione finora
- Female Reproductive SystemDocumento40 pagineFemale Reproductive SystemSAYMABANUNessuna valutazione finora
- Female Reproductive System (Yuni)Documento36 pagineFemale Reproductive System (Yuni)Ayi Abdul BasithNessuna valutazione finora
- (Mebooksfree Net) Cor&pro&pla&sur&nel&buc&2nd PDFDocumento527 pagine(Mebooksfree Net) Cor&pro&pla&sur&nel&buc&2nd PDFCucos Natalia100% (1)
- Hialuronidaza PDFDocumento8 pagineHialuronidaza PDFCucos NataliaNessuna valutazione finora
- Essentials of Plastic Surgery, 2nd EditionDocumento1.351 pagineEssentials of Plastic Surgery, 2nd EditionIcleanu Alexandru84% (19)
- 16 ISS Baker Haddon 1974Documento10 pagine16 ISS Baker Haddon 1974Parnil SinghNessuna valutazione finora
- Menstrual Disorders Associated With Thyroid Dysfunction: Ramya M. R., Parvathavarthini, Darshan Savery, R. SankareswariDocumento5 pagineMenstrual Disorders Associated With Thyroid Dysfunction: Ramya M. R., Parvathavarthini, Darshan Savery, R. SankareswariCucos NataliaNessuna valutazione finora
- Amputation Stumps H. E.: Harding Langdale-Kelham, London, EnglandDocumento3 pagineAmputation Stumps H. E.: Harding Langdale-Kelham, London, EnglandCucos NataliaNessuna valutazione finora
- 04 Rasulic Acta 1Documento6 pagine04 Rasulic Acta 1Cucos NataliaNessuna valutazione finora
- Essentials of Plastic Surgery, 2nd EditionDocumento1.351 pagineEssentials of Plastic Surgery, 2nd EditionIcleanu Alexandru84% (19)
- NeliganDocumento1.404 pagineNeliganCucos Natalia100% (2)
- Neuroma of HandDocumento5 pagineNeuroma of HandCucos NataliaNessuna valutazione finora
- Surgical Treatment of Strabismus in AdultsDocumento1 paginaSurgical Treatment of Strabismus in AdultsCucos NataliaNessuna valutazione finora
- Alogrefele de NerviDocumento11 pagineAlogrefele de NerviCucos NataliaNessuna valutazione finora
- Leziunea de Peroneu ComunDocumento16 pagineLeziunea de Peroneu ComunCucos NataliaNessuna valutazione finora
- Brachial PlexusDocumento42 pagineBrachial PlexusPrince DuNessuna valutazione finora
- Apk Retention Exam RevieweeDocumento9 pagineApk Retention Exam RevieweeKennie RamirezNessuna valutazione finora
- Cervical RadiculopathyDocumento7 pagineCervical Radiculopathyrhymescsf100% (1)
- 2014-10-17 Trail Guide To The Body CH 2Documento4 pagine2014-10-17 Trail Guide To The Body CH 2Ben WisherNessuna valutazione finora
- The Way of Thinking in Brachial Plexus InjuryDocumento48 pagineThe Way of Thinking in Brachial Plexus InjuryYoonHeeNyNessuna valutazione finora
- Physical Therapy Protocols For Conditions of Shoulder RegionDocumento111 paginePhysical Therapy Protocols For Conditions of Shoulder RegionPieng Napa100% (1)
- L3 AP 101 Mock Questions Exam Guide V101.2Documento24 pagineL3 AP 101 Mock Questions Exam Guide V101.2Sergiu TitcuNessuna valutazione finora
- Massage Therapy For Bruxism, TMJ SyndromeDocumento39 pagineMassage Therapy For Bruxism, TMJ SyndromeAdam Kesher100% (1)
- MRMDocumento39 pagineMRMZafirnur Amrin JasmanNessuna valutazione finora
- Brachial Plexus PowerpointDocumento32 pagineBrachial Plexus PowerpointZulkarnain Syamsuri100% (1)
- Anatomy 1 - MSS (Upper Limb)Documento127 pagineAnatomy 1 - MSS (Upper Limb)Abdullah As'adNessuna valutazione finora
- Acumed® Clavicle PlatingDocumento68 pagineAcumed® Clavicle Platingthomsoon01Nessuna valutazione finora
- Breast Anatomy and Mammography PositioningDocumento38 pagineBreast Anatomy and Mammography Positioningjitendra guptaNessuna valutazione finora
- Assessing The Breasts and Axillae: DelegationDocumento4 pagineAssessing The Breasts and Axillae: DelegationVioletteNessuna valutazione finora
- Anatomy 1.4 Upper Limbs - Muscle and FasciaDocumento10 pagineAnatomy 1.4 Upper Limbs - Muscle and Fascialovelots1234Nessuna valutazione finora
- Neuro Handbook (SUNY)Documento100 pagineNeuro Handbook (SUNY)Serge KhelemsKy100% (3)
- Mnemonics - AnatomyDocumento3 pagineMnemonics - Anatomymastac741Nessuna valutazione finora
- Anatomy Mnemonics UsmleDocumento65 pagineAnatomy Mnemonics UsmleHoney HoneyNessuna valutazione finora
- The Shoulder GirdleDocumento26 pagineThe Shoulder GirdleVeena VishwanathNessuna valutazione finora
- Master Degree in Plastic Surgery ThesisDocumento117 pagineMaster Degree in Plastic Surgery ThesisMohamed Ahmed El-RoubyNessuna valutazione finora
- Anatomy - Pectoral Region and Axilla PDFDocumento4 pagineAnatomy - Pectoral Region and Axilla PDFAngel KimNessuna valutazione finora
- Lambou Delto PectoralDocumento9 pagineLambou Delto PectoralalexNessuna valutazione finora
- Brachial PlexusDocumento62 pagineBrachial PlexusTutankhamoun Akhenatoun100% (2)
- Univ of Michigan - Gross Anatomy - Muscles TablesDocumento41 pagineUniv of Michigan - Gross Anatomy - Muscles TablesDarren Lim100% (1)
- BreastDocumento27 pagineBreastRasha HelmyNessuna valutazione finora
- History ExaminationDocumento18 pagineHistory ExaminationMohammed FaragNessuna valutazione finora
- 01 Muscles of The Chest WallDocumento10 pagine01 Muscles of The Chest WallAlvaro Mantilla GarcíaNessuna valutazione finora
- Touch For Health Level IDocumento2 pagineTouch For Health Level ISilvia De AlejandroNessuna valutazione finora
- Serdev Suture Techniques Breast Lift - Prof Nikolay P Serdev MD PHDDocumento4 pagineSerdev Suture Techniques Breast Lift - Prof Nikolay P Serdev MD PHDjobetobaNessuna valutazione finora
- Muscles of The Back Region - Listed Alphabetically Muscle Origin Insertion Action Innervation Artery NotesDocumento32 pagineMuscles of The Back Region - Listed Alphabetically Muscle Origin Insertion Action Innervation Artery NotesMaria Celina Lomboy SerapioNessuna valutazione finora