Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
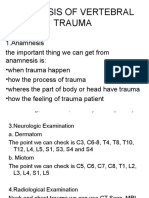
- Diagnosis of Vertebral TraumaDocumento2 pagineDiagnosis of Vertebral TraumaIka SriNessuna valutazione finora
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- 1cardiovascular PharmacologyDocumento20 pagine1cardiovascular PharmacologyIka SriNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- 1Documento1 pagina1Ika SriNessuna valutazione finora
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- What Exactly Is Uterine Prolapse?Documento3 pagineWhat Exactly Is Uterine Prolapse?Ika SriNessuna valutazione finora
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Aspek HemostasisDocumento23 pagineAspek HemostasisIka SriNessuna valutazione finora
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- SM 4-20080522-Kbk-Drug Induced Allergy and Hypersensitivity FinalDocumento32 pagineSM 4-20080522-Kbk-Drug Induced Allergy and Hypersensitivity FinalIka SriNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hansson Pin System Brochure P002 28 20131023Documento24 pagineHansson Pin System Brochure P002 28 20131023ElenaNessuna valutazione finora
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Psych Units 11-13 Cheat SheetDocumento1 paginaPsych Units 11-13 Cheat SheetTalia ShumanNessuna valutazione finora
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- 19-06-2017-10-15-0416257 - PD - VMO - Cardiology - Ryde HospitalDocumento8 pagine19-06-2017-10-15-0416257 - PD - VMO - Cardiology - Ryde HospitalHassamNessuna valutazione finora
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- General PharmacologyDocumento8 pagineGeneral PharmacologysekarenthangavelNessuna valutazione finora
- Nitrous Oxide in Emergency MedicineDocumento4 pagineNitrous Oxide in Emergency MedicinenumaidecatNessuna valutazione finora
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Bryan 3-24-17Documento12 pagineBryan 3-24-17Bryan VandentoornNessuna valutazione finora
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- How To Perform A Head To Toe AssessmentDocumento2 pagineHow To Perform A Head To Toe AssessmentLalaine RomeroNessuna valutazione finora
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Journal Ivp-WPS OfficeDocumento8 pagineJournal Ivp-WPS OfficeDyahtripNessuna valutazione finora
- Times Leader 03-17-2013Documento77 pagineTimes Leader 03-17-2013The Times LeaderNessuna valutazione finora
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- Grasp Manual11492Documento12 pagineGrasp Manual11492Fariya Hamid CFNessuna valutazione finora
- HELLO! Magazine Laser Eye Surgery ArticleDocumento1 paginaHELLO! Magazine Laser Eye Surgery ArticleLondon Vision ClinicNessuna valutazione finora
- WCU NURS 491L - Integration of Nursing Practice - 2014fall - I - 8-4-14Documento29 pagineWCU NURS 491L - Integration of Nursing Practice - 2014fall - I - 8-4-14Joseph MeyerNessuna valutazione finora
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- 4 Sedation Care PolicyDocumento5 pagine4 Sedation Care PolicyFarah Andleeb MalikNessuna valutazione finora
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- Episodic SOAP Note Template - RX PedsDocumento11 pagineEpisodic SOAP Note Template - RX PedsBrianne Foster75% (4)
- Adl IadlDocumento20 pagineAdl IadlKrisna Eka Yudha100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Drugs Affecting The Gastrointestinal SystemDocumento5 pagineDrugs Affecting The Gastrointestinal SystemPaul André AzcunaNessuna valutazione finora
- Medical Marijuana PresentationDocumento19 pagineMedical Marijuana Presentationsudheer vamarajuNessuna valutazione finora
- Professional Services, Inc. vs. NatividadDocumento13 pagineProfessional Services, Inc. vs. NatividadEarleen Del RosarioNessuna valutazione finora
- Drug Tariff Workshop 13-14 - StudentDocumento10 pagineDrug Tariff Workshop 13-14 - StudentCrystal Sia Yiik SwanNessuna valutazione finora
- Final - HOSPITAL BILL FORMAT PDFDocumento2 pagineFinal - HOSPITAL BILL FORMAT PDFH C85% (13)
- Introduction To StatisticsDocumento6 pagineIntroduction To StatisticsMangala SemageNessuna valutazione finora
- 6mwt Protocol FinalDocumento7 pagine6mwt Protocol FinalSara Rodríguez SeoaneNessuna valutazione finora
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Emergency RadiologyDocumento79 pagineEmergency RadiologyRahul Yadav100% (3)
- Therapeutic CommunicationDocumento82 pagineTherapeutic CommunicationYvette Vallejo100% (2)
- MSN FP6216 ForsythKathryn Assessment4 2Documento6 pagineMSN FP6216 ForsythKathryn Assessment4 2NbiNessuna valutazione finora
- Clinical Nursing Manual PDFDocumento93 pagineClinical Nursing Manual PDFVatau FlorinNessuna valutazione finora
- EsmololDocumento3 pagineEsmololTri Purma SariNessuna valutazione finora
- Medel SonataDocumento54 pagineMedel Sonatamaclab macNessuna valutazione finora
- Temporary Flexible Removable Partial DentureDocumento4 pagineTemporary Flexible Removable Partial DentureenipurwantiNessuna valutazione finora
- Alcohol ConcentrationDocumento5 pagineAlcohol Concentrationapi-299736788Nessuna valutazione finora
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)