Potrebbero piacerti anche
- PathoLec InflammationDocumento10 paginePathoLec InflammationMiguel Cuevas DolotNessuna valutazione finora
- Pathology Week 2 p1-18Documento18 paginePathology Week 2 p1-18zeroun24100% (1)
- Inflammation & Immune ResponseDocumento68 pagineInflammation & Immune ResponseAgata Krisensia Putri100% (1)
- Acute and Chronic InflammationDocumento22 pagineAcute and Chronic InflammationRedhwan85Nessuna valutazione finora
- Macromolecules WorksheetDocumento6 pagineMacromolecules WorksheetMyka Zoldyck0% (1)
- Acute InflammationDocumento55 pagineAcute InflammationMohammad_Islam8790% (10)
- Acute and Chronic Inflammation: Yacob Alemu (MD) May 2021Documento89 pagineAcute and Chronic Inflammation: Yacob Alemu (MD) May 2021Tazeb AyeleNessuna valutazione finora
- Inflammation and Wound HealingDocumento46 pagineInflammation and Wound HealingVijetha RaiNessuna valutazione finora
- Acute InflammationDocumento64 pagineAcute InflammationSuleiman KikulweNessuna valutazione finora
- Vitamin C Ascorbic AcidDocumento21 pagineVitamin C Ascorbic Acidapi-388948078Nessuna valutazione finora
- Chapter 45 Hormones and The Endocrine SystemDocumento12 pagineChapter 45 Hormones and The Endocrine System蔡旻珊Nessuna valutazione finora
- Winkelman - Shamanism and The Origins of Spirituality and Ritual HealingDocumento32 pagineWinkelman - Shamanism and The Origins of Spirituality and Ritual Healinggustavo zelayaNessuna valutazione finora
- Inflammation and Tissue Repair: July 2021Documento54 pagineInflammation and Tissue Repair: July 2021EdenNessuna valutazione finora
- Andriani Daskalaki-Handbook of Research On Systems Biology Applications in Medicine (2008)Documento917 pagineAndriani Daskalaki-Handbook of Research On Systems Biology Applications in Medicine (2008)Алексей Почтилейтинантзапаса100% (2)
- Acute and Chronic InflamationDocumento59 pagineAcute and Chronic InflamationLeni ruslainiNessuna valutazione finora
- Inflammation. Etiology. Vascular Changes. Cellular Events in Inflammation. Acute Inflammation. Morphologic PatternsDocumento57 pagineInflammation. Etiology. Vascular Changes. Cellular Events in Inflammation. Acute Inflammation. Morphologic PatternsZauzaNessuna valutazione finora
- Inflammation: Inflammation Is A Protective Response, The Goal of Which Is To EliminateDocumento26 pagineInflammation: Inflammation Is A Protective Response, The Goal of Which Is To EliminateDavid Cahyo WibisonoNessuna valutazione finora
- 2.INFLAMMATION AND ITS IMPLICATIONS ..... FinalDocumento81 pagine2.INFLAMMATION AND ITS IMPLICATIONS ..... Finalsaloni singhNessuna valutazione finora
- A Inflammation For NursingDocumento47 pagineA Inflammation For NursingSintayehu MulatuNessuna valutazione finora
- Inflammation and Repair-2021Documento93 pagineInflammation and Repair-2021Manav VyasNessuna valutazione finora
- InflammationDocumento17 pagineInflammationNajwa AbdualgaderNessuna valutazione finora
- Inflammation Seminar WordDocumento19 pagineInflammation Seminar WordDrGurinder Kanwar100% (1)
- InflammationDocumento48 pagineInflammationTewodros TeshomeNessuna valutazione finora
- Inflammation and Tissue RepairDocumento55 pagineInflammation and Tissue RepairSingitan SiyoumNessuna valutazione finora
- Lecture 4 Unit II BPT PathologyDocumento16 pagineLecture 4 Unit II BPT PathologySudip ShresthaNessuna valutazione finora
- Acute and Chronic InflammationDocumento69 pagineAcute and Chronic InflammationJac mswimaNessuna valutazione finora
- 1 Acute InflammationDocumento6 pagine1 Acute InflammationNauzaina IjazNessuna valutazione finora
- 2.4 2.5 Radang Akut Kronik Dan MorfologiDocumento51 pagine2.4 2.5 Radang Akut Kronik Dan MorfologimeNessuna valutazione finora
- لقطة شاشة ٢٠٢٣-١١-٠٩ في ٨.٥٣.٥٠ صDocumento7 pagineلقطة شاشة ٢٠٢٣-١١-٠٩ في ٨.٥٣.٥٠ صmo44hh44Nessuna valutazione finora
- 2017 - Inflammation & Hamodinamic DisorderDocumento93 pagine2017 - Inflammation & Hamodinamic Disorder숭숩Nessuna valutazione finora
- 07 InflammationDocumento69 pagine07 InflammationSangameswaran B.BNessuna valutazione finora
- SHS 301 Lect-05Documento44 pagineSHS 301 Lect-05AAZEEN ALINessuna valutazione finora
- INFLAMAATIONDocumento6 pagineINFLAMAATIONSabbir AhmedNessuna valutazione finora
- Inflammation. Part 1. Fall 2022.Documento60 pagineInflammation. Part 1. Fall 2022.Mirleyka GonzálezNessuna valutazione finora
- Appendicitis Meningitis: Vascular Cellular Response The Inflammatory Process RepairDocumento10 pagineAppendicitis Meningitis: Vascular Cellular Response The Inflammatory Process RepairYaff DthNessuna valutazione finora
- Harsh Mohan Quick Review InflammationDocumento23 pagineHarsh Mohan Quick Review InflammationTanaya PujareNessuna valutazione finora
- Study-Notes - Inflammation-And-Repair (1) 88Documento17 pagineStudy-Notes - Inflammation-And-Repair (1) 88jjjkkNessuna valutazione finora
- 2.acute & Chronic Inflammation, S1Documento90 pagine2.acute & Chronic Inflammation, S1LennyOctaviaNessuna valutazione finora
- Acute InflammationDocumento76 pagineAcute InflammationOmor faruk HridoyNessuna valutazione finora
- Inflammation and RepairDocumento34 pagineInflammation and Repairanshum guptaNessuna valutazione finora
- Pathology Book - Chapter 2 - Inflammation - HKDocumento12 paginePathology Book - Chapter 2 - Inflammation - HKagar agarNessuna valutazione finora
- Inflammation For BDS StudentsDocumento24 pagineInflammation For BDS StudentsMohan Prasad GuptaNessuna valutazione finora
- Inflammation NotesDocumento12 pagineInflammation NotesavidadarkestevillearnNessuna valutazione finora
- InflammationDocumento8 pagineInflammationGhazi Uddin AhmedNessuna valutazione finora
- Lecture 3Documento56 pagineLecture 3w2tz2qrqxdNessuna valutazione finora
- Session 08 Acute InflammationDocumento40 pagineSession 08 Acute Inflammationkasper mkNessuna valutazione finora
- Handout On InflammationDocumento76 pagineHandout On InflammationlydNessuna valutazione finora
- Inflammation NotesDocumento12 pagineInflammation Noteskarthikeyan rajeevNessuna valutazione finora
- Inflamasi Akut Dan KronikDocumento60 pagineInflamasi Akut Dan KronikDhea Resty PratiwiNessuna valutazione finora
- InflammationDocumento2 pagineInflammationSujan BoseNessuna valutazione finora
- Immunology of Inflammation - SlidesDocumento22 pagineImmunology of Inflammation - SlidesEssington BeloNessuna valutazione finora
- InflammationDocumento8 pagineInflammationHarjot RandhawaNessuna valutazione finora
- Patogenesis Infeksi Bakteri, Infeksi Lokal, Dan SepsisDocumento52 paginePatogenesis Infeksi Bakteri, Infeksi Lokal, Dan SepsisNia AnestyaNessuna valutazione finora
- Inflammation & Immune ResponseDocumento68 pagineInflammation & Immune Responsesuday sunday100% (1)
- InflammationDocumento22 pagineInflammationAhmad Khan GhoriNessuna valutazione finora
- 2 InflammationDocumento91 pagine2 InflammationDesta BelachewNessuna valutazione finora
- Group No 3Documento19 pagineGroup No 3محمد نعیم اقبالNessuna valutazione finora
- InflammationDocumento117 pagineInflammationPraiseNessuna valutazione finora
- Acute and Chronic InflammationDocumento40 pagineAcute and Chronic InflammationIqra ChNessuna valutazione finora
- PATHOLOGYDocumento16 paginePATHOLOGYSahara MahatNessuna valutazione finora
- InflammationDocumento83 pagineInflammationpriyaNessuna valutazione finora
- Inflamasi Akut Dan KronikDocumento60 pagineInflamasi Akut Dan KronikMunawir_Syam91Nessuna valutazione finora
- Acute InflammationDocumento76 pagineAcute InflammationMuhammad Modu BulamaNessuna valutazione finora
- For Mucocele Lesions - Careful Excisional BiopsyDocumento11 pagineFor Mucocele Lesions - Careful Excisional BiopsyBibek RajNessuna valutazione finora
- Curriculum Vitae: Personal DetailsDocumento3 pagineCurriculum Vitae: Personal DetailsBibek RajNessuna valutazione finora
- QDWPlicDocumento2 pagineQDWPlicBibek RajNessuna valutazione finora
- Practical Skill Station Basic Life Support Key Teaching ObjectivesDocumento3 paginePractical Skill Station Basic Life Support Key Teaching ObjectivesBibek RajNessuna valutazione finora
- JdsmcxnksDocumento32 pagineJdsmcxnksBibek RajNessuna valutazione finora
- When Is Oral Biopsy Not Needed?Documento6 pagineWhen Is Oral Biopsy Not Needed?Bibek RajNessuna valutazione finora
- 3 UhnjkcDocumento8 pagine3 UhnjkcBibek RajNessuna valutazione finora
- DrtfygbyuijDocumento29 pagineDrtfygbyuijBibek RajNessuna valutazione finora
- Biopsy Is Derived From A Greek Word (By-Op-See) Bio - Meaning LIFE and Opsy - TO LOOK (Vision)Documento5 pagineBiopsy Is Derived From A Greek Word (By-Op-See) Bio - Meaning LIFE and Opsy - TO LOOK (Vision)Bibek RajNessuna valutazione finora
- JDJDJDJDocumento23 pagineJDJDJDJBibek RajNessuna valutazione finora
- Background Triads Framework: Jan Clarkson, Craig Ramsay, Linda Young, Paula Elouafkaoui and Heather CassieDocumento1 paginaBackground Triads Framework: Jan Clarkson, Craig Ramsay, Linda Young, Paula Elouafkaoui and Heather CassieBibek RajNessuna valutazione finora
- DhdifogkDocumento4 pagineDhdifogkBibek RajNessuna valutazione finora
- Trapezoidal Flap. A Diagrammatic IllustrationDocumento6 pagineTrapezoidal Flap. A Diagrammatic IllustrationBibek RajNessuna valutazione finora
- Vitamin B-Functions, Food Sources and RDA Value Deficiency and Their Oral ManifestationsDocumento6 pagineVitamin B-Functions, Food Sources and RDA Value Deficiency and Their Oral ManifestationsBibek RajNessuna valutazione finora
- Toothbrushing Chart PDFDocumento1 paginaToothbrushing Chart PDFBibek RajNessuna valutazione finora
- YudsbhcjDocumento1 paginaYudsbhcjBibek RajNessuna valutazione finora
- FfghhthjgvyujhDocumento1 paginaFfghhthjgvyujhBibek RajNessuna valutazione finora
- Background Methods: Review' (OHAR) Guidance in BriefDocumento1 paginaBackground Methods: Review' (OHAR) Guidance in BriefBibek RajNessuna valutazione finora
- Ultrasonic Cleaner Test Record: Ultrasonic Serial Number - LocationDocumento2 pagineUltrasonic Cleaner Test Record: Ultrasonic Serial Number - LocationBibek RajNessuna valutazione finora
- YuybnunhhuhbDocumento2 pagineYuybnunhhuhbBibek RajNessuna valutazione finora
- VfyggdbDocumento33 pagineVfyggdbBibek RajNessuna valutazione finora
- Warfarin and Your Dental Treatment: Information For PatientsDocumento5 pagineWarfarin and Your Dental Treatment: Information For PatientsBibek RajNessuna valutazione finora
- TG 6 YhunjDocumento48 pagineTG 6 YhunjBibek RajNessuna valutazione finora
- Dental Anxiety Form 4 PDFDocumento2 pagineDental Anxiety Form 4 PDFBibek RajNessuna valutazione finora
- Rapid: Reducing Antibiotic Prescribing in DentistryDocumento5 pagineRapid: Reducing Antibiotic Prescribing in DentistryBibek RajNessuna valutazione finora
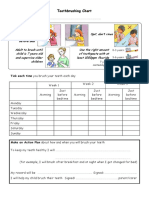
- Toothbrushing Chart: Tick Each Time You Brush Your Teeth Each DayDocumento1 paginaToothbrushing Chart: Tick Each Time You Brush Your Teeth Each DayBibek RajNessuna valutazione finora
- Patient's Name:: Ms. Bharti PorwalDocumento1 paginaPatient's Name:: Ms. Bharti PorwalHimanshuNessuna valutazione finora
- About MangrovesDocumento5 pagineAbout MangrovesKathleen Laum CabanlitNessuna valutazione finora
- From Start To Phase 1 in 30 Months - Insilico MedicineDocumento9 pagineFrom Start To Phase 1 in 30 Months - Insilico MedicinejeanNessuna valutazione finora
- The Detritus Food-Web and The Diversity of Soil Fauna As Indicators of Disturbance Regimes in Agro-EcosystemsDocumento9 pagineThe Detritus Food-Web and The Diversity of Soil Fauna As Indicators of Disturbance Regimes in Agro-EcosystemsFábio Luís MostassoNessuna valutazione finora
- DNA Sequencing by Capillary Electrophoresis Chemistry GuideDocumento310 pagineDNA Sequencing by Capillary Electrophoresis Chemistry GuidepicapenasNessuna valutazione finora
- Discuss Genetic Factors in AggressionDocumento2 pagineDiscuss Genetic Factors in AggressionmopheadfattyNessuna valutazione finora
- General Zoology Module 1 Arthropoda and EchinodermataDocumento5 pagineGeneral Zoology Module 1 Arthropoda and EchinodermataPaul PanizaNessuna valutazione finora
- Worksheet - Metabolism Seventh GradeDocumento2 pagineWorksheet - Metabolism Seventh Gradeerika alzateNessuna valutazione finora
- ! Genetica - Curs + LPDocumento740 pagine! Genetica - Curs + LPTobei AchimNessuna valutazione finora
- HHS Public Access: BRAT1 Mutations Present With A Spectrum of Clinical SeverityDocumento16 pagineHHS Public Access: BRAT1 Mutations Present With A Spectrum of Clinical SeveritykroleminiNessuna valutazione finora
- 3rd Summative Test in Science - 4 Name: - Score: - Teacher: - SchoolDocumento2 pagine3rd Summative Test in Science - 4 Name: - Score: - Teacher: - SchoolManelyn Taga100% (3)
- MBS 331 BiochemistryDocumento23 pagineMBS 331 BiochemistryChris Francis CiaNessuna valutazione finora
- Bacitracin Disks: Interpretation of ResultsDocumento2 pagineBacitracin Disks: Interpretation of ResultsOsama BakheetNessuna valutazione finora
- Winter Course Allocation Report (Updated On 18dec2015)Documento274 pagineWinter Course Allocation Report (Updated On 18dec2015)ASEEMNessuna valutazione finora
- IMPORTANTVan de Ven and Poole (1995)Documento32 pagineIMPORTANTVan de Ven and Poole (1995)stefi1234Nessuna valutazione finora
- Photosynthesis (KEY)Documento6 paginePhotosynthesis (KEY)kylevNessuna valutazione finora
- Recombinant Human Hyaluronidase PH20Documento1 paginaRecombinant Human Hyaluronidase PH20Iva ColterNessuna valutazione finora
- The Five Kingdom Classification System ArticleDocumento3 pagineThe Five Kingdom Classification System ArticleNermine AbedNessuna valutazione finora
- Biotic Stree and Yield LossDocumento258 pagineBiotic Stree and Yield LossDhanraj KumarNessuna valutazione finora
- Reproduction 3Documento7 pagineReproduction 3Shweta JainNessuna valutazione finora
- Keragaman Jeruk Fungsional Indonesia Berdasarkan Karakter Morfologis Dan Marka RAPDDocumento10 pagineKeragaman Jeruk Fungsional Indonesia Berdasarkan Karakter Morfologis Dan Marka RAPDUlfahNessuna valutazione finora
- 7 week:: Microbial Growth (미생물의 성장)Documento24 pagine7 week:: Microbial Growth (미생물의 성장)MoonHoLeeNessuna valutazione finora
- MCQ FMS4 2009 FixDocumento18 pagineMCQ FMS4 2009 Fixdanielgunawan92Nessuna valutazione finora
- Bioremediation of PesticidesDocumento3 pagineBioremediation of PesticidesSunil VohraNessuna valutazione finora
- Molecules Are DNA Molecules Formed by Laboratory Methods of Genetic RecombinationDocumento2 pagineMolecules Are DNA Molecules Formed by Laboratory Methods of Genetic RecombinationMarygrace Broñola100% (2)