Potrebbero piacerti anche
- Calculous Biliary DiseaseDocumento71 pagineCalculous Biliary DiseaseMinnossNessuna valutazione finora
- Gastrointestinal EndosDocumento28 pagineGastrointestinal EndosAqeel AhmedNessuna valutazione finora
- Gastric Carcinoma: H. Pylori InfectionDocumento7 pagineGastric Carcinoma: H. Pylori InfectionMuvenn KannanNessuna valutazione finora
- Perforated Peptic Ulcer - An UpdateDocumento17 paginePerforated Peptic Ulcer - An UpdateRama_Aditya_KNessuna valutazione finora
- Gastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDa EverandGastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNessuna valutazione finora
- Colorectal CancerDocumento29 pagineColorectal CancerLeeyanBhadzzVagayNessuna valutazione finora
- SMALL INTESTINE QuickDocumento8 pagineSMALL INTESTINE QuickErald PaderangaNessuna valutazione finora
- Ascitic Fluid AnalysisDocumento3 pagineAscitic Fluid AnalysisLohJNessuna valutazione finora
- Cholangitis: Reported By: R. DongaranDocumento18 pagineCholangitis: Reported By: R. DongaranVishnu Karunakaran100% (1)
- Case Protocol Kawasaki DiseaseDocumento5 pagineCase Protocol Kawasaki DiseaseFranz SalazarNessuna valutazione finora
- Large Bowel Obstruction by Nic MDocumento42 pagineLarge Bowel Obstruction by Nic MRisky OpponentNessuna valutazione finora
- Complication of Peptic Ulcer: Department of Surgery S. S. Medical College Rewa and Associate GMH and SGMH RewaDocumento76 pagineComplication of Peptic Ulcer: Department of Surgery S. S. Medical College Rewa and Associate GMH and SGMH RewaBrajesh MouryaNessuna valutazione finora
- Case AppendicitisDocumento30 pagineCase AppendicitisSarahNessuna valutazione finora
- 21 Obstructive JaundiceDocumento12 pagine21 Obstructive JaundicejumaymayaNessuna valutazione finora
- Cme Acs 2. Stemi (Izzah)Documento36 pagineCme Acs 2. Stemi (Izzah)Hakimah K. SuhaimiNessuna valutazione finora
- Prostate CancerDocumento6 pagineProstate CancerfheisanzNessuna valutazione finora
- Acute PeritonitisDocumento4 pagineAcute PeritonitisSatrio Tri HadmokoNessuna valutazione finora
- Hepatocellular Carcinoma: Hepatocellular Carcinoma (HCC, Also Called Malignant Hepatoma) Is The MostDocumento10 pagineHepatocellular Carcinoma: Hepatocellular Carcinoma (HCC, Also Called Malignant Hepatoma) Is The MostNurul An NisaNessuna valutazione finora
- Appendectomy GuidelinesDocumento12 pagineAppendectomy GuidelinesJessa Frances FranciscoNessuna valutazione finora
- Pancretic Cancer Case Study - BurkeDocumento52 paginePancretic Cancer Case Study - Burkeapi-282999254Nessuna valutazione finora
- Upper Gi BleedDocumento20 pagineUpper Gi BleedNaeem Shehzad100% (1)
- Aetiology, Pathology and Management of Enterocutaneous FistulaDocumento34 pagineAetiology, Pathology and Management of Enterocutaneous Fistularoselinekhadija100% (1)
- Pancreatic Cancer: Aziz Ahmad, MD Surgical Oncology Mills-Peninsula Hospital April 23, 2011Documento18 paginePancreatic Cancer: Aziz Ahmad, MD Surgical Oncology Mills-Peninsula Hospital April 23, 2011mywifenoor1983Nessuna valutazione finora
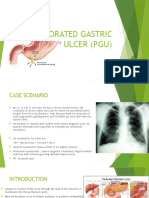
- Perforated Gastric Ulcer (Pgu)Documento10 paginePerforated Gastric Ulcer (Pgu)Jen NeeNessuna valutazione finora
- Whipple Procedure Case Study PresentationDocumento30 pagineWhipple Procedure Case Study Presentationapi-315408947100% (3)
- HematuriaDocumento42 pagineHematuriaWasim R. IssaNessuna valutazione finora
- Case Presentation Lump Right HypochondriumDocumento22 pagineCase Presentation Lump Right HypochondriumNANDAN RAINessuna valutazione finora
- Appendicitis in Children Vineyard (Dr. Faisol)Documento28 pagineAppendicitis in Children Vineyard (Dr. Faisol)Alinta AyuningtyasNessuna valutazione finora
- Gastric Carcinoma: Professor Ravi KantDocumento44 pagineGastric Carcinoma: Professor Ravi KantDaniel Alfredo Tenorio GonzálezNessuna valutazione finora
- Anorectal MalformationsDocumento6 pagineAnorectal Malformationskhadzx100% (2)
- Paper Presentation On Trichobezoars A Hairy Cause of Intestinal ObstructionDocumento14 paginePaper Presentation On Trichobezoars A Hairy Cause of Intestinal ObstructionAimanNessuna valutazione finora
- Mass in Epigastrium-2Documento37 pagineMass in Epigastrium-2brown_chocolate87643100% (1)
- Colorectal Ca PresentationDocumento25 pagineColorectal Ca Presentationapi-399299717Nessuna valutazione finora
- Phimosis and ParaphimosisDocumento3 paginePhimosis and ParaphimosisJoshua PowersNessuna valutazione finora
- Cholecystitis & Carcinoma of GallbladderDocumento37 pagineCholecystitis & Carcinoma of GallbladderSalsabila Al-Basheer100% (1)
- Renal TumorsDocumento38 pagineRenal TumorsMim Rashed0% (1)
- PancreatitisDocumento51 paginePancreatitisMizrab NadeemNessuna valutazione finora
- Acute AbdomenDocumento24 pagineAcute AbdomenGrace SimmonsNessuna valutazione finora
- A Giant Juvenile Fibroadenoma of BreastDocumento2 pagineA Giant Juvenile Fibroadenoma of BreastIOSRjournalNessuna valutazione finora
- IntussusceptionDocumento33 pagineIntussusceptionNovendi RizkaNessuna valutazione finora
- Perforated Peptic UlcerDocumento68 paginePerforated Peptic UlcerSaibo BoldsaikhanNessuna valutazione finora
- Gall Stone Disease: DR M.farhad General SurgeonDocumento56 pagineGall Stone Disease: DR M.farhad General SurgeondrelvNessuna valutazione finora
- Medical Case of SurgeryDocumento7 pagineMedical Case of SurgerysugisweNessuna valutazione finora
- CholangitisDocumento15 pagineCholangitisFaye TanNessuna valutazione finora
- Jaundice: Seminar Under The Guidance Of-Dr. Shiva NarangDocumento47 pagineJaundice: Seminar Under The Guidance Of-Dr. Shiva NarangMiguel MansillaNessuna valutazione finora
- Case Presentation Meyke Liechandra C11109130 Fracture ClavicleDocumento24 pagineCase Presentation Meyke Liechandra C11109130 Fracture ClavicleWahyunita IlhamNessuna valutazione finora
- Gastric Outlet Obstruction (Stenosis) : Lior Shlomov 1852Documento8 pagineGastric Outlet Obstruction (Stenosis) : Lior Shlomov 1852Lior ShlomovNessuna valutazione finora
- UGIBDocumento34 pagineUGIBChe Ainil ZainodinNessuna valutazione finora
- Adenocarcinoma of The Colon and RectumDocumento49 pagineAdenocarcinoma of The Colon and RectumMunawar AliNessuna valutazione finora
- ERCPDocumento11 pagineERCPMalaak BassamNessuna valutazione finora
- Problem-based Approach to Gastroenterology and HepatologyDa EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNessuna valutazione finora
- Presentation 1Documento71 paginePresentation 1http_uglyNessuna valutazione finora
- CholangitisDocumento20 pagineCholangitisNikoFebriRyandoNessuna valutazione finora
- Achalasia KSDocumento40 pagineAchalasia KSPridho GaziansyahNessuna valutazione finora
- Upper GIT BleedingDocumento69 pagineUpper GIT BleedingSoleh Ramly100% (1)
- Case of Obstructive JaundiceDocumento38 pagineCase of Obstructive JaundiceadiNessuna valutazione finora
- 6.examination of Inguinal SwellingDocumento4 pagine6.examination of Inguinal SwellingMuvenn Kannan100% (1)
- Acute Abdominal Pain MS LectureDocumento63 pagineAcute Abdominal Pain MS Lectureheka_amrongNessuna valutazione finora
- Acute Gastroenteritis (AGE)Documento37 pagineAcute Gastroenteritis (AGE)Sari HariyaniNessuna valutazione finora
- BlepharitisDocumento20 pagineBlepharitisNorshahidah IedaNessuna valutazione finora
- Norshahidah Binti Zainal SD012017-04-002565Documento15 pagineNorshahidah Binti Zainal SD012017-04-002565Norshahidah IedaNessuna valutazione finora
- Case Study BlepharitisDocumento12 pagineCase Study BlepharitisNorshahidah IedaNessuna valutazione finora
- Management of HypoglycemiaDocumento14 pagineManagement of HypoglycemiaNorshahidah IedaNessuna valutazione finora
- CELLUTISDocumento16 pagineCELLUTISNorshahidah Ieda0% (1)
- Breast Cancer (Abi)Documento15 pagineBreast Cancer (Abi)Norshahidah IedaNessuna valutazione finora
- GDMDocumento16 pagineGDMNorshahidah IedaNessuna valutazione finora
- AsthaDocumento16 pagineAsthaNorshahidah IedaNessuna valutazione finora
- Femur Midshaft FractureDocumento18 pagineFemur Midshaft FractureNorshahidah Ieda100% (1)
- Brain AbscessDocumento22 pagineBrain AbscessNorshahidah IedaNessuna valutazione finora
- Hydro Cep Hal UsDocumento35 pagineHydro Cep Hal UsNorshahidah IedaNessuna valutazione finora
- Anaemia in PregnancyDocumento15 pagineAnaemia in PregnancyNorshahidah Ieda100% (1)
- Breast Cancer (Abi)Documento15 pagineBreast Cancer (Abi)Norshahidah IedaNessuna valutazione finora
- Perforated Gastric UlcerDocumento18 paginePerforated Gastric UlcerNorshahidah IedaNessuna valutazione finora
- Control and PreventionDocumento11 pagineControl and PreventionNorshahidah IedaNessuna valutazione finora
- GDMDocumento17 pagineGDMNorshahidah IedaNessuna valutazione finora
- Perforated Gastric UlcerDocumento15 paginePerforated Gastric UlcerNorshahidah IedaNessuna valutazione finora
- The Effectiveness of Communication Among HealthcarDocumento24 pagineThe Effectiveness of Communication Among HealthcarNorshahidah IedaNessuna valutazione finora
- Traction Application ShaDocumento6 pagineTraction Application ShaNorshahidah IedaNessuna valutazione finora
- AnaemiaDocumento15 pagineAnaemiaNorshahidah IedaNessuna valutazione finora
- Effects of Parental Divorce Among Student/Teenagers: Norshahidah Zainal SD012017-04-002565 Dma Sept 2015Documento20 pagineEffects of Parental Divorce Among Student/Teenagers: Norshahidah Zainal SD012017-04-002565 Dma Sept 2015Norshahidah IedaNessuna valutazione finora
- Breast CancerDocumento15 pagineBreast CancerNorshahidah IedaNessuna valutazione finora
- Presentation Management Trainee Batch VII - Mohammad Arian RahmatullahDocumento8 paginePresentation Management Trainee Batch VII - Mohammad Arian RahmatullahMohammad Arian RahmatullahNessuna valutazione finora
- 13 19 PBDocumento183 pagine13 19 PBmaxim reinerNessuna valutazione finora
- Devi Strotam PDFDocumento9 pagineDevi Strotam PDFDiary Of A Wise ManNessuna valutazione finora
- 17.5 Return On Investment and Compensation ModelsDocumento20 pagine17.5 Return On Investment and Compensation ModelsjamieNessuna valutazione finora
- Mythbusters - Archimedes Cannon QuestionsDocumento2 pagineMythbusters - Archimedes Cannon QuestionsVictoria RojugbokanNessuna valutazione finora
- Hydrostatic PressureDocumento13 pagineHydrostatic Pressureapi-2859151810% (1)
- Case Digest 1-4.46Documento4 pagineCase Digest 1-4.46jobelle barcellanoNessuna valutazione finora
- The Myth of HITLER's POPE - Hubert - LunsDocumento13 pagineThe Myth of HITLER's POPE - Hubert - LunsHubert LunsNessuna valutazione finora
- Aptitude TestDocumento19 pagineAptitude TestSANANessuna valutazione finora
- Online Sales of New Cars: StudyDocumento29 pagineOnline Sales of New Cars: StudyIson StudiosNessuna valutazione finora
- Tristan TateDocumento3 pagineTristan Tatecelebritydecks1Nessuna valutazione finora
- Lantolf Concept Based InstructionDocumento16 pagineLantolf Concept Based Instructionphdreadings39Nessuna valutazione finora
- Utah GFL Interview Answers TableDocumento5 pagineUtah GFL Interview Answers TableKarsten WalkerNessuna valutazione finora
- Two Steps From Hell Full Track ListDocumento13 pagineTwo Steps From Hell Full Track ListneijeskiNessuna valutazione finora
- Suitcase Lady Christie Mclaren ThesisDocumento7 pagineSuitcase Lady Christie Mclaren ThesisWriteMyPaperForMeCheapNewHaven100% (2)
- The Discovery of The Tun Huang Library and Its Effect On Chinese StudiesDocumento21 pagineThe Discovery of The Tun Huang Library and Its Effect On Chinese Studiesfabricatore_21639575Nessuna valutazione finora
- The Wall Dramaturgical PacketDocumento24 pagineThe Wall Dramaturgical PacketMarilo CostaNessuna valutazione finora
- B. Concept of The State - PeopleDocumento2 pagineB. Concept of The State - PeopleLizanne GauranaNessuna valutazione finora
- Experimental Nucleonics PDFDocumento1 paginaExperimental Nucleonics PDFEricNessuna valutazione finora
- Impulse: Operation ManualDocumento8 pagineImpulse: Operation ManualRonggo SukmoNessuna valutazione finora
- Taoism: Michelle Azutea Lei Llabres Laurisse Anne Magpayo Juniel Tuazon Zaldy Bryan BajadaDocumento26 pagineTaoism: Michelle Azutea Lei Llabres Laurisse Anne Magpayo Juniel Tuazon Zaldy Bryan Bajadana2than-1Nessuna valutazione finora
- Types of Communicative StrategyDocumento46 pagineTypes of Communicative StrategyMyra Bolinas100% (1)
- SkripsiDocumento101 pagineSkripsiNurul Maharani PutriNessuna valutazione finora
- Haiti Research Project 2021Documento3 pagineHaiti Research Project 2021api-518908670Nessuna valutazione finora
- Presentation 1Documento7 paginePresentation 1Funio KhanNessuna valutazione finora
- Diabetes Mellitus in Pediatric: Dr. Wasnaa Hadi AbdullahDocumento30 pagineDiabetes Mellitus in Pediatric: Dr. Wasnaa Hadi AbdullahLily AddamsNessuna valutazione finora
- A Beginner's Guide To Reading Jung - Jungian Center For The Spiritual SciencesDocumento6 pagineA Beginner's Guide To Reading Jung - Jungian Center For The Spiritual SciencesRosa ChacónNessuna valutazione finora
- Kashida Embroidery: KashmirDocumento22 pagineKashida Embroidery: KashmirRohit kumarNessuna valutazione finora
- (2017) (Enfield) Distributed AgencyDocumento305 pagine(2017) (Enfield) Distributed Agencyjose100% (1)
- Systematic Survey On Smart Home Safety and Security Systems Using The Arduino PlatformDocumento24 pagineSystematic Survey On Smart Home Safety and Security Systems Using The Arduino PlatformGeri MaeNessuna valutazione finora