Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (400)
- Protocol For Blunt Abdominal TraumaDocumento19 pagineProtocol For Blunt Abdominal TraumaabigailNessuna valutazione finora
- Appendix A: Doppler Ultrasound and Ankle-Brachial Pressure IndexDocumento26 pagineAppendix A: Doppler Ultrasound and Ankle-Brachial Pressure IndexabigailNessuna valutazione finora
- Wellness PlannerDocumento12 pagineWellness PlannerabigailNessuna valutazione finora
- Januar Y2021: Sunday Monday Tuesday Wednesday Thur Sday FR I Day Sat UrdayDocumento12 pagineJanuar Y2021: Sunday Monday Tuesday Wednesday Thur Sday FR I Day Sat UrdayabigailNessuna valutazione finora
- Royal Australasian College of Surgeons Research, Audit and Academic SurgeryDocumento18 pagineRoyal Australasian College of Surgeons Research, Audit and Academic SurgeryabigailNessuna valutazione finora
- January2020: SUN MON TUE WED THU FRI SATDocumento12 pagineJanuary2020: SUN MON TUE WED THU FRI SATabigailNessuna valutazione finora
- Peer Evaluation FormDocumento1 paginaPeer Evaluation FormabigailNessuna valutazione finora
- Journal of Neurosurgery Management of Peripheral Nerve SheathDocumento9 pagineJournal of Neurosurgery Management of Peripheral Nerve SheathabigailNessuna valutazione finora
- (Atlases of Clinical Nuclear Medicine) Harvey A. Ziessman (Auth.) Harvey ADocumento182 pagine(Atlases of Clinical Nuclear Medicine) Harvey A. Ziessman (Auth.) Harvey AabigailNessuna valutazione finora
- (Blueprints Series) Seth J. Karp MD James P.G. Morris MD - Blueprints SurgDocumento279 pagine(Blueprints Series) Seth J. Karp MD James P.G. Morris MD - Blueprints Surgabigail100% (1)
- Our Eye As A Camera Refraction, Errors and Solutions.: DR - Ali.A.Taqi Fifth Year StudentsDocumento44 pagineOur Eye As A Camera Refraction, Errors and Solutions.: DR - Ali.A.Taqi Fifth Year Studentsabigail100% (1)
- 1 - Aldea Neighborhood Rules Regulations Revised 2021-06-28Documento15 pagine1 - Aldea Neighborhood Rules Regulations Revised 2021-06-28abigailNessuna valutazione finora
- Antidiabetic Drugs 2Documento52 pagineAntidiabetic Drugs 2abigailNessuna valutazione finora
- Approach To Abdominal Pain: Dr. Nahla A Azzam MRCP Consultant GastroenterologyDocumento28 pagineApproach To Abdominal Pain: Dr. Nahla A Azzam MRCP Consultant GastroenterologySurat SaengjindaNessuna valutazione finora
- FinlandDocumento6 pagineFinlandabigailNessuna valutazione finora
- The Power of PrayerDocumento5 pagineThe Power of PrayerabigailNessuna valutazione finora
- Preventive MedicineDocumento10 paginePreventive MedicineHuji JalamiNessuna valutazione finora
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (121)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Anger, Rage, and Hatred: A Powerpoint PresentationDocumento20 pagineAnger, Rage, and Hatred: A Powerpoint PresentationJane GilgunNessuna valutazione finora
- MBA Coaching and Institutes IndiaDocumento2 pagineMBA Coaching and Institutes IndiamakemycareerNessuna valutazione finora
- WEEK 3 LessonDocumento17 pagineWEEK 3 LessonadscoNessuna valutazione finora
- Classification and ClusteringDocumento8 pagineClassification and ClusteringDivya GNessuna valutazione finora
- DLP Mapeh G7Documento2 pagineDLP Mapeh G7HannahNessuna valutazione finora
- Teaching Pragmatics of GreetingsDocumento10 pagineTeaching Pragmatics of Greetingsابو محمدNessuna valutazione finora
- Reviewer in RWSDocumento6 pagineReviewer in RWSAbraham Del CastilloNessuna valutazione finora
- BACC 2 Human Resource Management OBTLDocumento16 pagineBACC 2 Human Resource Management OBTLNelvin VallesNessuna valutazione finora
- TEACHERS AND STUDENTS' PERCEPTIONS OF A Goog Teacher of EnglishDocumento57 pagineTEACHERS AND STUDENTS' PERCEPTIONS OF A Goog Teacher of Englishgiangmilk0812100% (1)
- Rubric b2 Writing InteractiveDocumento1 paginaRubric b2 Writing Interactiveanuska81Nessuna valutazione finora
- Technology For Teaching and Learning in The Elementary GradesDocumento7 pagineTechnology For Teaching and Learning in The Elementary GradesAlyssa AlegadoNessuna valutazione finora
- EBP Power Point Rubric Austin GayDocumento2 pagineEBP Power Point Rubric Austin GayMadison ThomasNessuna valutazione finora
- Essay Writing (English) - Soksay ClubDocumento2 pagineEssay Writing (English) - Soksay ClubNica BinaraoNessuna valutazione finora
- Critical ThinkingDocumento8 pagineCritical ThinkingSarah NaderNessuna valutazione finora
- English 9 Efdt 3Documento6 pagineEnglish 9 Efdt 3John Mark PascoNessuna valutazione finora
- Inquiry-Based Science Learning 2Documento41 pagineInquiry-Based Science Learning 2Joseph ShapiraNessuna valutazione finora
- Giao An Tieng Anh 6 I Learn Smart World Hoc Ki 1Documento201 pagineGiao An Tieng Anh 6 I Learn Smart World Hoc Ki 1NhanNessuna valutazione finora
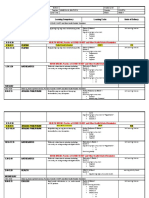
- Weekly Home Learning Plan Day and Time Learning Area Learning Competency Learning Tasks Mode of Delivery Monday 8:00-9:15 FilipinoDocumento5 pagineWeekly Home Learning Plan Day and Time Learning Area Learning Competency Learning Tasks Mode of Delivery Monday 8:00-9:15 FilipinoVanessa BautistaNessuna valutazione finora
- Addressing Overcrowding in School CanteensDocumento5 pagineAddressing Overcrowding in School Canteenshzlynmnlnsn14100% (1)
- Cooperative Learning in Language Education - George Jacobs & Willy RenandyaDocumento81 pagineCooperative Learning in Language Education - George Jacobs & Willy RenandyaBảoo NguyễnNessuna valutazione finora
- Semi-Detailed Lesson PlanDocumento2 pagineSemi-Detailed Lesson PlanKaycee Eecyak86% (7)
- Scope and LimitationDocumento5 pagineScope and Limitationmark33% (3)
- Bilingual and Bilingual Education Colin BakerDocumento18 pagineBilingual and Bilingual Education Colin BakerEdgar AguirreNessuna valutazione finora
- Ptcas Personal StatementDocumento2 paginePtcas Personal Statementapi-277000361Nessuna valutazione finora
- Ass 2 EntrepDocumento4 pagineAss 2 EntrepEzra Cedriec DumayasNessuna valutazione finora
- Short Title - IBS.: Module - Introduction To Business Studies (IBS)Documento21 pagineShort Title - IBS.: Module - Introduction To Business Studies (IBS)beni benoNessuna valutazione finora
- Strategic Directions Fy 2017-2022Documento20 pagineStrategic Directions Fy 2017-2022GJ BadenasNessuna valutazione finora
- The Effects of The Constructivist Learning Approach On StudentDocumento14 pagineThe Effects of The Constructivist Learning Approach On StudentkonzertarienNessuna valutazione finora
- Chapter 001 Introduction Strategic HRM in The Twenty - First CenturyDocumento14 pagineChapter 001 Introduction Strategic HRM in The Twenty - First CenturyOsamah FahadNessuna valutazione finora
- The Challenges of Implementing Project-Based Learning in Middle SchoolsDocumento133 pagineThe Challenges of Implementing Project-Based Learning in Middle SchoolsraneeNessuna valutazione finora