Potrebbero piacerti anche
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDa EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeValutazione: 4 su 5 stelle4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDa EverandThe Little Book of Hygge: Danish Secrets to Happy LivingValutazione: 3.5 su 5 stelle3.5/5 (399)
- Aph PPH - 0 PDFDocumento81 pagineAph PPH - 0 PDFSherlyn YeeNessuna valutazione finora
- Dysphagia: Departemen THT-KL Fakultas Kedokteran Universitas Padjadjaran 2016Documento31 pagineDysphagia: Departemen THT-KL Fakultas Kedokteran Universitas Padjadjaran 2016Sherlyn YeeNessuna valutazione finora
- Leukocyte DisordersDocumento55 pagineLeukocyte DisordersSherlyn Yee100% (1)
- Mechanisme LaborDocumento31 pagineMechanisme LaborSherlyn YeeNessuna valutazione finora
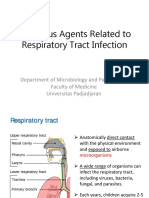
- Microbial Aspect of URTI MLDocumento63 pagineMicrobial Aspect of URTI MLSherlyn YeeNessuna valutazione finora
- CSS DHFDocumento6 pagineCSS DHFSherlyn YeeNessuna valutazione finora
- UveitisDocumento17 pagineUveitisSherlyn Yee100% (1)
- Inguinal Hernia: From Wikipedia, The Free EncyclopediaDocumento6 pagineInguinal Hernia: From Wikipedia, The Free EncyclopediaSherlyn YeeNessuna valutazione finora
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDa EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryValutazione: 3.5 su 5 stelle3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDa EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceValutazione: 4 su 5 stelle4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Da EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Valutazione: 4 su 5 stelle4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDa EverandShoe Dog: A Memoir by the Creator of NikeValutazione: 4.5 su 5 stelle4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDa EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureValutazione: 4.5 su 5 stelle4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDa EverandNever Split the Difference: Negotiating As If Your Life Depended On ItValutazione: 4.5 su 5 stelle4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDa EverandGrit: The Power of Passion and PerseveranceValutazione: 4 su 5 stelle4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDa EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaValutazione: 4.5 su 5 stelle4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDa EverandThe Emperor of All Maladies: A Biography of CancerValutazione: 4.5 su 5 stelle4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDa EverandOn Fire: The (Burning) Case for a Green New DealValutazione: 4 su 5 stelle4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDa EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersValutazione: 4.5 su 5 stelle4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDa EverandTeam of Rivals: The Political Genius of Abraham LincolnValutazione: 4.5 su 5 stelle4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDa EverandThe Unwinding: An Inner History of the New AmericaValutazione: 4 su 5 stelle4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDa EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyValutazione: 3.5 su 5 stelle3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDa EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreValutazione: 4 su 5 stelle4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Da EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Valutazione: 4.5 su 5 stelle4.5/5 (119)
- Her Body and Other Parties: StoriesDa EverandHer Body and Other Parties: StoriesValutazione: 4 su 5 stelle4/5 (821)
- Vaccines CircaDocumento10 pagineVaccines CircamariavillaresNessuna valutazione finora
- Different Types of Diseases/disorders of The Nervous System.Documento23 pagineDifferent Types of Diseases/disorders of The Nervous System.Saba Parvin Haque100% (4)
- Acupressure Massage For AscitesDocumento4 pagineAcupressure Massage For Ascitessaif ahmedNessuna valutazione finora
- Cholecystectomy Nursing Care Plan: Risk For InfectionDocumento1 paginaCholecystectomy Nursing Care Plan: Risk For InfectionBesael BaccolNessuna valutazione finora
- Abortion Complications - Background, Pathophysiology, EtiologyDocumento4 pagineAbortion Complications - Background, Pathophysiology, EtiologyAldair SanchezNessuna valutazione finora
- Antibiotic Guidelines For AdultsDocumento9 pagineAntibiotic Guidelines For AdultsVarshini Tamil SelvanNessuna valutazione finora
- New Flu Shot Approved by FDADocumento6 pagineNew Flu Shot Approved by FDAHaraprasad NanjundappaNessuna valutazione finora
- Deesha Bhaumik CV PHD Apps For 889Documento3 pagineDeesha Bhaumik CV PHD Apps For 889api-533748985Nessuna valutazione finora
- Crao PosterDocumento1 paginaCrao PosterNataShini RajaRatnamNessuna valutazione finora
- Social Pharmacy Practical 1Documento35 pagineSocial Pharmacy Practical 1Devam VanjariNessuna valutazione finora
- Karol The Great Plague 15 01 15Documento4 pagineKarol The Great Plague 15 01 15api-276953527Nessuna valutazione finora
- Does Drinking Coffee Really Bad for Health? The Benefits Outweigh the RisksDocumento1 paginaDoes Drinking Coffee Really Bad for Health? The Benefits Outweigh the Riskswahyu kencanaNessuna valutazione finora
- Homework: 1) What Does The Respiratory System Do ?Documento6 pagineHomework: 1) What Does The Respiratory System Do ?Mariana VasileNessuna valutazione finora
- Kamus Icd 10 Dan Icd 9Documento10 pagineKamus Icd 10 Dan Icd 9trisnawati100% (1)
- King Abdulaziz University College of Pharmacy Clinical PharmacyDocumento3 pagineKing Abdulaziz University College of Pharmacy Clinical PharmacyHusnain AhmadNessuna valutazione finora
- AnthraxDocumento40 pagineAnthraxAnjana BalakrishnanNessuna valutazione finora
- Epa HQ Opp 2016 0385 0094 PDFDocumento227 pagineEpa HQ Opp 2016 0385 0094 PDFuncleadolphNessuna valutazione finora
- CefalexinDocumento1 paginaCefalexinIvan Matthew SuperioNessuna valutazione finora
- COVID-19 consumable products catalogDocumento2 pagineCOVID-19 consumable products catalogRadit AMSNessuna valutazione finora
- Coronavirus FactsheetDocumento8 pagineCoronavirus FactsheetJm2345234029Nessuna valutazione finora
- National Acupuncture Foundation - Clean Needle Technique Ver PDFDocumento73 pagineNational Acupuncture Foundation - Clean Needle Technique Ver PDFJessé de AndradeNessuna valutazione finora
- HIV/AIDS Awareness Seminar ReactionDocumento4 pagineHIV/AIDS Awareness Seminar ReactionStefanny Anne GuminangNessuna valutazione finora
- COVID-19 Vaccine Mechanisms and ImmunityDocumento1 paginaCOVID-19 Vaccine Mechanisms and ImmunityAvinash KumbharNessuna valutazione finora
- Jurnal MalabsorbsiDocumento6 pagineJurnal MalabsorbsiIda Putri IhsaniNessuna valutazione finora
- BC COMPLICATIONS & PROGNOSISDocumento42 pagineBC COMPLICATIONS & PROGNOSISalalmaee1Nessuna valutazione finora
- Final Exam National Board of Examinations JUNE 2020 Cardiology Paper-Iii Time: 3 Hours CARD/J/20/05/III MAX. MARKS: 100 Important InstructionsDocumento1 paginaFinal Exam National Board of Examinations JUNE 2020 Cardiology Paper-Iii Time: 3 Hours CARD/J/20/05/III MAX. MARKS: 100 Important InstructionsnarasimhahanNessuna valutazione finora
- Adam VitalDocumento5 pagineAdam VitalAdam Vital HospitalNessuna valutazione finora
- Ettinger 2005Documento7 pagineEttinger 2005Santy P Vásconez CalderónNessuna valutazione finora
- Func - Samplebooklet - Libro Gratis de Muestra Pivot PointDocumento81 pagineFunc - Samplebooklet - Libro Gratis de Muestra Pivot PointRaquel100% (1)
- Ccort AtlasDocumento240 pagineCcort Atlasjacazio.brischettoNessuna valutazione finora