Potrebbero piacerti anche
- Seminar: Daniel P Webster, Paul Klenerman, Geoff Rey M DusheikoDocumento12 pagineSeminar: Daniel P Webster, Paul Klenerman, Geoff Rey M Dusheikovira khairunisaNessuna valutazione finora
- HIVDocumento79 pagineHIVMehiella SatchiNessuna valutazione finora
- Pathogenic Mechanisms in HBV-and HCV-associated Hepatocellular CarcinomaDocumento13 paginePathogenic Mechanisms in HBV-and HCV-associated Hepatocellular CarcinomaJosé MateusNessuna valutazione finora
- Medical Virology: Dr. Dalia M. Mohsen Prof. in MicrobiologyDocumento43 pagineMedical Virology: Dr. Dalia M. Mohsen Prof. in MicrobiologyDalia M. MohsenNessuna valutazione finora
- Hepatitis C Virus: Screening, Diagnosis, and Interpretation of Laboratory AssaysDocumento8 pagineHepatitis C Virus: Screening, Diagnosis, and Interpretation of Laboratory AssaysCristafeNessuna valutazione finora
- Module 5. AIDSDocumento21 pagineModule 5. AIDSShreya JindalNessuna valutazione finora
- Gulu Cohes Hiv Nelly MDDocumento68 pagineGulu Cohes Hiv Nelly MDYIKI ISAACNessuna valutazione finora
- Epidemiology, Pathogenesis and Management of HIV Infection in Patients with Periodontal DiseaseDocumento27 pagineEpidemiology, Pathogenesis and Management of HIV Infection in Patients with Periodontal Diseasemin moongNessuna valutazione finora
- Hepatitis C: by DR Faiza SamadDocumento44 pagineHepatitis C: by DR Faiza SamadMuhammad MakkiNessuna valutazione finora
- Rubella Virus, Congenital Syndrome and Hepatitis C TreatmentDocumento43 pagineRubella Virus, Congenital Syndrome and Hepatitis C TreatmentBatool SherbiniNessuna valutazione finora
- Hepatitis B, C and DDocumento13 pagineHepatitis B, C and DMehiella SatchiNessuna valutazione finora
- HIV/AIDS in Kenya: Key Facts, Statistics and Prevention MethodsDocumento7 pagineHIV/AIDS in Kenya: Key Facts, Statistics and Prevention MethodsSusan HepziNessuna valutazione finora
- Viral Hepatitis ReadingDocumento51 pagineViral Hepatitis ReadingNadya VanessaNessuna valutazione finora
- HIV SeminarDocumento111 pagineHIV SeminarRakshaNessuna valutazione finora
- WHO Global Action Strategy 2011Documento24 pagineWHO Global Action Strategy 2011Ameena AimenNessuna valutazione finora
- Hepatitis BDocumento12 pagineHepatitis BTeti AndriNessuna valutazione finora
- Smith 2020Documento10 pagineSmith 2020senaNessuna valutazione finora
- Public Health Immigration and Viral HepatitisDocumento8 paginePublic Health Immigration and Viral HepatitisEdgar MejiaNessuna valutazione finora
- Management of Acute Hepatitis B PDFDocumento17 pagineManagement of Acute Hepatitis B PDFMary CogolloNessuna valutazione finora
- Hiv/Aids: by Aisha MansurDocumento34 pagineHiv/Aids: by Aisha MansurMpanso Ahmad AlhijjNessuna valutazione finora
- Hiv and Hepatitis BDocumento8 pagineHiv and Hepatitis BShree Narayan YadavNessuna valutazione finora
- Nursing Care in AIDSDocumento18 pagineNursing Care in AIDSInsaniNessuna valutazione finora
- Public Health Immigration and Viral HepatitisDocumento8 paginePublic Health Immigration and Viral HepatitisFenny Noor AidaNessuna valutazione finora
- HIV/AIDS Structure, Transmission, and StagesDocumento22 pagineHIV/AIDS Structure, Transmission, and StagesJireh MejinoNessuna valutazione finora
- Diagnosis and Treatment of Chronic Hepatitis B: Raymond D'Souza Graham R FosterDocumento4 pagineDiagnosis and Treatment of Chronic Hepatitis B: Raymond D'Souza Graham R FosterrayNessuna valutazione finora
- Chronic Viral Hepatitis BDocumento24 pagineChronic Viral Hepatitis BАлина ЛентицкийNessuna valutazione finora
- Text Book of Microbiology (221-330)Documento110 pagineText Book of Microbiology (221-330)Jamila ridaNessuna valutazione finora
- Transmission and prevention of hepatitis virusesDocumento35 pagineTransmission and prevention of hepatitis virusesANUAR ASISNessuna valutazione finora
- Current Perioperative Management of The Patient With Hiv A B, H M, C R, A G, A K e A.M. FDocumento12 pagineCurrent Perioperative Management of The Patient With Hiv A B, H M, C R, A G, A K e A.M. FPrashant SinghNessuna valutazione finora
- Hepatology - 2014 - Messina - Global Distribution and Prevalence of Hepatitis C Virus GenotypesDocumento11 pagineHepatology - 2014 - Messina - Global Distribution and Prevalence of Hepatitis C Virus GenotypesDem tksNessuna valutazione finora
- WHO Position Paper HepBDocumento9 pagineWHO Position Paper HepBpradipkshetriNessuna valutazione finora
- Ijmsv02p0050 PDFDocumento8 pagineIjmsv02p0050 PDFfikaanugrahNessuna valutazione finora
- Hiv Infection and AidsDocumento51 pagineHiv Infection and Aidspokhara gharipatanNessuna valutazione finora
- Hepathology VHCDocumento11 pagineHepathology VHCMaria Fernanda LopezNessuna valutazione finora
- Medical Progress: H C V IDocumento16 pagineMedical Progress: H C V IriahNessuna valutazione finora
- Immunology of Hepatitis B Virus and Hepatitis C Virus InfectionDocumento15 pagineImmunology of Hepatitis B Virus and Hepatitis C Virus InfectionMark BowlerNessuna valutazione finora
- Infection Control LecturDocumento62 pagineInfection Control LecturMoona WahabNessuna valutazione finora
- Pathogen Safety Data Sheet1 HCVDocumento8 paginePathogen Safety Data Sheet1 HCVAsel AselNessuna valutazione finora
- HIVBlood Borne Virus Infections MMC GuidelineDocumento24 pagineHIVBlood Borne Virus Infections MMC GuidelinePalanivelu VijayakumarNessuna valutazione finora
- Human Immunodeficiency Virus (HIV) and Acquired Immunodeficiency Syndrome (AIDS)Documento6 pagineHuman Immunodeficiency Virus (HIV) and Acquired Immunodeficiency Syndrome (AIDS)Vanessa MolinaNessuna valutazione finora
- Khvi 17 1819742Documento24 pagineKhvi 17 1819742Sebastian BurgosNessuna valutazione finora
- PM - Materi 1 HIV AIDS RevDocumento72 paginePM - Materi 1 HIV AIDS RevSaly AlatasNessuna valutazione finora
- AidsDocumento35 pagineAidsCiarie PerezNessuna valutazione finora
- HIV/AIDS Learning GuideDocumento130 pagineHIV/AIDS Learning GuideRoline KarimiNessuna valutazione finora
- Hiv/Aids and Principles of HaartDocumento88 pagineHiv/Aids and Principles of Haarthabtamu alemayehuNessuna valutazione finora
- Medical Progress: H C V IDocumento16 pagineMedical Progress: H C V ITrisya Bella FibriantiNessuna valutazione finora
- Nihms 839861Documento40 pagineNihms 839861Faisal JamshedNessuna valutazione finora
- Hepatitis Delta Infection - Current and New Treatment OptionsDocumento7 pagineHepatitis Delta Infection - Current and New Treatment OptionsDiana Carolina di Filippo VillaNessuna valutazione finora
- Viral Hepatitis & HIVDocumento14 pagineViral Hepatitis & HIVaymnhssn2020Nessuna valutazione finora
- Peac Hiv-2Documento31 paginePeac Hiv-2SdNessuna valutazione finora
- Microbiolog Y: Your Health. Our MissionDocumento61 pagineMicrobiolog Y: Your Health. Our MissionAbdellatef HossamNessuna valutazione finora
- Hcca Rev Nri 2005Documento15 pagineHcca Rev Nri 2005Patrick RamosNessuna valutazione finora
- Hepatitis B: Hepatitis B Is An Infectious Illness of The Liver Caused by The Hepatitis B Virus (HBV) That Affects ApesDocumento3 pagineHepatitis B: Hepatitis B Is An Infectious Illness of The Liver Caused by The Hepatitis B Virus (HBV) That Affects ApesSyeda BismaNessuna valutazione finora
- Seminar: Christian Trépo, Henry L Y Chan, Anna LokDocumento11 pagineSeminar: Christian Trépo, Henry L Y Chan, Anna LokGERALDINE JARAMILLO VARGASNessuna valutazione finora
- 3 HIV PresentationDocumento22 pagine3 HIV PresentationMaiCAlmanzorNessuna valutazione finora
- HEPATITIS B EpidemiologyDocumento14 pagineHEPATITIS B Epidemiologytarun_apr25Nessuna valutazione finora
- FP2 (Pak Hasyim) Human Immunodeficiency Virus (HIV) and AcquiredDocumento19 pagineFP2 (Pak Hasyim) Human Immunodeficiency Virus (HIV) and Acquiredaha ehe ohoNessuna valutazione finora
- Management of The Patient With HIV DeseaseDocumento34 pagineManagement of The Patient With HIV DeseaseTeresa MontesNessuna valutazione finora
- Stages of HIV Infection and AIDS ExplainedDocumento10 pagineStages of HIV Infection and AIDS ExplainedHarshitha Gowda HarshiNessuna valutazione finora
- Introduction to Respiratory Syncytial Virus InfectionDa EverandIntroduction to Respiratory Syncytial Virus InfectionNessuna valutazione finora
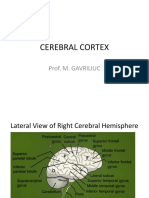
- 13 Cerebral CortexDocumento85 pagine13 Cerebral CortexIon UngureanuNessuna valutazione finora
- LICHIDUL CEFALORAHIDIAN ANALIZADocumento5 pagineLICHIDUL CEFALORAHIDIAN ANALIZACezaraJalencoNessuna valutazione finora
- HSV Encephalitis Diagnosis and TreatmentDocumento23 pagineHSV Encephalitis Diagnosis and TreatmentIon BurlacuNessuna valutazione finora
- The Autonomic Nervous SystemDocumento59 pagineThe Autonomic Nervous SystemRita ErmuracheNessuna valutazione finora
- Modern Classification and Causes of Headaches and Facial PainsDocumento53 pagineModern Classification and Causes of Headaches and Facial PainsIon UngureanuNessuna valutazione finora
- Atlas Gray's PDFDocumento403 pagineAtlas Gray's PDFIon UngureanuNessuna valutazione finora
- Sobotta - Atlas Human Anatomy Volume1 14th Edition (WWW - Irananatomy.ir) PDFDocumento426 pagineSobotta - Atlas Human Anatomy Volume1 14th Edition (WWW - Irananatomy.ir) PDFIoana Alexandra100% (1)
- Atlas de Anatomie A Omului McMinnDocumento340 pagineAtlas de Anatomie A Omului McMinnoana_4u_89702495% (110)
- Atlas de Anatomie A Omului McMinnDocumento340 pagineAtlas de Anatomie A Omului McMinnoana_4u_89702495% (110)
- Evaluarea Practica in Pediatrie (Scan C.a.)Documento67 pagineEvaluarea Practica in Pediatrie (Scan C.a.)Ion Ungureanu100% (1)
- LICHIDUL CEFALORAHIDIAN ANALIZADocumento5 pagineLICHIDUL CEFALORAHIDIAN ANALIZACezaraJalencoNessuna valutazione finora
- Understanding Chronic Viral Hepatitis CDocumento37 pagineUnderstanding Chronic Viral Hepatitis CIon UngureanuNessuna valutazione finora
- Digestive System PathophysiologyDocumento16 pagineDigestive System PathophysiologyCamryn NewellNessuna valutazione finora
- Pfizer R&D Pipeline As of February 2008Documento20 paginePfizer R&D Pipeline As of February 2008jennabush100% (1)
- Non Invasive Imaging in NASHDocumento3 pagineNon Invasive Imaging in NASHParul SoodNessuna valutazione finora
- Hi Jam ADocumento12 pagineHi Jam Aelan sudjanamihardja100% (4)
- Cholangiocarcinoma: Adeel S. Khan,, Leigh Anne DagefordeDocumento21 pagineCholangiocarcinoma: Adeel S. Khan,, Leigh Anne DagefordeCirugía General HEVESNessuna valutazione finora
- FibroscanDocumento3 pagineFibroscanAri WirantariNessuna valutazione finora
- Laboratory ValuesDocumento12 pagineLaboratory ValuesJaney Co100% (2)
- Community Health Final Exam ReviewDocumento4 pagineCommunity Health Final Exam ReviewkcharmaigneNessuna valutazione finora
- Nonalcoholic Steatohepatitis. Review JAMA March 2020Documento9 pagineNonalcoholic Steatohepatitis. Review JAMA March 2020Luis Henrique SalesNessuna valutazione finora
- Postmortem Diagnosis of Esophageal Variceal BleedingDocumento3 paginePostmortem Diagnosis of Esophageal Variceal BleedingClaudia MoldovanuNessuna valutazione finora
- Brunner Answer KeyDocumento13 pagineBrunner Answer KeyMaria Luisa Villaluna100% (2)
- Nelson EmbriologiDocumento88 pagineNelson Embriologisheryn pujionoNessuna valutazione finora
- Hepatitis: Jump To Navigation Jump To SearchDocumento11 pagineHepatitis: Jump To Navigation Jump To SearchZely ApriantiNessuna valutazione finora
- LIVER CHIRROSIS and GERED QUESTION AND ANSWERSDocumento10 pagineLIVER CHIRROSIS and GERED QUESTION AND ANSWERSjess_nookieNessuna valutazione finora
- Chirosis Hepatic PDFDocumento8 pagineChirosis Hepatic PDFCikalHrNessuna valutazione finora
- Liver: Presented by Dr. Tahmina Islam MD Third PartDocumento121 pagineLiver: Presented by Dr. Tahmina Islam MD Third PartNajib JamilNessuna valutazione finora
- Liver Cirrhosis - NCPDocumento18 pagineLiver Cirrhosis - NCPIshmael Solamillo83% (6)
- Cirrhosis Hepatis 1Documento48 pagineCirrhosis Hepatis 1Muhammad RivaileNessuna valutazione finora
- ACG Clinical Guideline Alcoholic Liver Disease.9Documento20 pagineACG Clinical Guideline Alcoholic Liver Disease.9Gopal Kumar DasNessuna valutazione finora
- Non-Alcoholic Fatty Liver Disease (NAFLD) : A Review of Epidemiology, Risk Factors, Diagnosis and ManagementDocumento16 pagineNon-Alcoholic Fatty Liver Disease (NAFLD) : A Review of Epidemiology, Risk Factors, Diagnosis and Managementdekatria 2020Nessuna valutazione finora
- Liver Cirrhosis NCPDocumento21 pagineLiver Cirrhosis NCPJeco Valdez100% (4)
- 2020 Gastro - Annc Format PDFDocumento4 pagine2020 Gastro - Annc Format PDFhalikalifhayaNessuna valutazione finora
- Abdominal Ultrasound - LiverDocumento30 pagineAbdominal Ultrasound - Liverpunct_org3256Nessuna valutazione finora
- FibroScan Physician Slideset 1.11.2016Documento37 pagineFibroScan Physician Slideset 1.11.2016Prudhvi Krishna Reddy100% (1)
- Chalasani Et Al 2018 HepatologyDocumento30 pagineChalasani Et Al 2018 HepatologyAlex DcostaNessuna valutazione finora
- Chronic Liver Disease Decompensated N PDFDocumento6 pagineChronic Liver Disease Decompensated N PDFmzhao230Nessuna valutazione finora
- Liver TransplantationDocumento13 pagineLiver TransplantationSaikat MitraNessuna valutazione finora
- Abnormal liver function and mildly coarse liver: Diagnosing and managing NASH cirrhosis complicationsDocumento38 pagineAbnormal liver function and mildly coarse liver: Diagnosing and managing NASH cirrhosis complicationsSandheepJanardhananNessuna valutazione finora
- Nutrition For Liver Gallbladder and Pancreas DiseasesDocumento39 pagineNutrition For Liver Gallbladder and Pancreas DiseasesMaricar Car CartallaNessuna valutazione finora
- Original1.Chapter 53 Surgical Complications of Cirrhosis and Portal HypertensionDocumento23 pagineOriginal1.Chapter 53 Surgical Complications of Cirrhosis and Portal Hypertensioncusom34Nessuna valutazione finora