Potrebbero piacerti anche
- Lung SurgeriesDocumento43 pagineLung SurgeriesSereinNessuna valutazione finora
- Canas, Patricia Gan, Razel Ruelo, Vanessa Aquino, Camile Guillano, Christabelle BSN IiiDocumento73 pagineCanas, Patricia Gan, Razel Ruelo, Vanessa Aquino, Camile Guillano, Christabelle BSN IiiGan BangNessuna valutazione finora
- Higher Center - Dr. BarbonDocumento5 pagineHigher Center - Dr. BarbonMelissa SalayogNessuna valutazione finora
- Cranial Nerve Exam in DetailDocumento36 pagineCranial Nerve Exam in DetailANIE100% (1)
- 15 CerebrumDocumento32 pagine15 CerebrumMédecin Adrian TGNessuna valutazione finora
- Origin & Conduction of Cardiac Impulse: Dr.S.Brinda MD Associate Professor PhysiologyDocumento36 pagineOrigin & Conduction of Cardiac Impulse: Dr.S.Brinda MD Associate Professor PhysiologyAtchaya ThillainatarajanNessuna valutazione finora
- Physiology of Limbic System by Dr. RoomiDocumento21 paginePhysiology of Limbic System by Dr. RoomiMudassar Roomi100% (3)
- Important Question of PhysiologyDocumento8 pagineImportant Question of PhysiologyRahul Yadav100% (2)
- PROPERTIES OF CARDIAC MUSCLEsDocumento16 paginePROPERTIES OF CARDIAC MUSCLEsHardik BagariaNessuna valutazione finora
- Internal CapsuleDocumento25 pagineInternal CapsuleMadan KumarNessuna valutazione finora
- Basics On NeurophysiologyDocumento12 pagineBasics On NeurophysiologyRausche Anne Blaser Sausa100% (1)
- Superficial and Deep ReflexesDocumento28 pagineSuperficial and Deep ReflexesShilpa SNessuna valutazione finora
- CSF and Blood Brain BarrierDocumento67 pagineCSF and Blood Brain BarrierPhysiology by Dr Raghuveer100% (1)
- Introduction To NeurophysiologyDocumento13 pagineIntroduction To Neurophysiologyvenkata ramakrishnaiahNessuna valutazione finora
- Erman Fandialan M.D. Department of Clinical Neurosciences UermmmcDocumento48 pagineErman Fandialan M.D. Department of Clinical Neurosciences Uermmmclovelots1234100% (1)
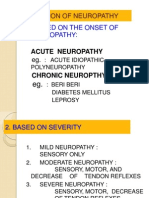
- Classification of NeuropathyDocumento16 pagineClassification of NeuropathysekiannNessuna valutazione finora
- 2006 PhysioDocumento18 pagine2006 Physioanaeshkl100% (1)
- Dermatomes & Myotomes PDFDocumento4 pagineDermatomes & Myotomes PDFsridhar_physio0% (1)
- ROM Booklet 07nov2010Documento26 pagineROM Booklet 07nov2010his.thunder122Nessuna valutazione finora
- General Surgery: Post-Operative Care and ManagementDocumento9 pagineGeneral Surgery: Post-Operative Care and ManagementMohammed Yousif AbdualjabbarNessuna valutazione finora
- The Motor System ExaminationDocumento42 pagineThe Motor System ExaminationHelend ChildDj100% (1)
- Cerebellum & Extra Pyramidal SystemDocumento33 pagineCerebellum & Extra Pyramidal SystemPhysio Saurav100% (1)
- HYDROCEPHALUSDocumento63 pagineHYDROCEPHALUSAjeng Aristiany Rahawarin100% (2)
- Anatomy & Physiology of The Cardiovascular SystemDocumento3 pagineAnatomy & Physiology of The Cardiovascular SystemluaNessuna valutazione finora
- Vitiligo PPT (1) .PPTX LectureDocumento35 pagineVitiligo PPT (1) .PPTX LectureVinay DhranaNessuna valutazione finora
- Blood Supply of BrainDocumento2 pagineBlood Supply of BrainvmagtotoNessuna valutazione finora
- How To Read XRay AbdomenDocumento65 pagineHow To Read XRay AbdomenKlinik KDU100% (1)
- IontophoresisDocumento4 pagineIontophoresisDr GowrishankarPotturi PTNessuna valutazione finora
- Wall Neuro 2010Documento34 pagineWall Neuro 2010Kath Jacinto100% (1)
- Lect.3, Properties of ReceptorsDocumento21 pagineLect.3, Properties of ReceptorsAttiqaQureshi100% (2)
- RomDocumento6 pagineRomPrivat Etavirp0% (1)
- Transverse MyelitisDocumento19 pagineTransverse MyelitisAnonymous YHQmN8a01100% (1)
- Biomechanics of Peripheral and Spinal Nerve RootsDocumento86 pagineBiomechanics of Peripheral and Spinal Nerve RootsJawad HassanNessuna valutazione finora
- Cervical RibDocumento15 pagineCervical RibArko duttaNessuna valutazione finora
- Nerve and Muscle PhysiologyDocumento82 pagineNerve and Muscle PhysiologychandsriNessuna valutazione finora
- Pleural EffusionDocumento78 paginePleural EffusionJessa AdenigNessuna valutazione finora
- BIOPSYDocumento8 pagineBIOPSYASHLEY DAWN BUENAFENessuna valutazione finora
- Neuromuscular and Nervous System 2010 With AnswersDocumento13 pagineNeuromuscular and Nervous System 2010 With AnswersWenzy CruzNessuna valutazione finora
- Thoracic Inlet Syndrome and Cervical RibDocumento28 pagineThoracic Inlet Syndrome and Cervical RibRabin DasNessuna valutazione finora
- Royal's Neurophysiology McqsDocumento17 pagineRoyal's Neurophysiology McqsJames IbrahimNessuna valutazione finora
- HeliotherapyDocumento20 pagineHeliotherapyDodo JuniorNessuna valutazione finora
- Ambulation Aids and Patterns 2018Documento59 pagineAmbulation Aids and Patterns 2018venkata ramakrishnaiah100% (1)
- Wrist Case Study 1Documento3 pagineWrist Case Study 1superhoofy7186100% (2)
- Anaesthesia For BPTDocumento38 pagineAnaesthesia For BPTBijeta ThapaNessuna valutazione finora
- Brain Anatomy and How The Brain WorksDocumento1 paginaBrain Anatomy and How The Brain Worksdudong borjaNessuna valutazione finora
- Assessing Neurologic System - FinalDocumento66 pagineAssessing Neurologic System - FinalAngelo EstanislaoNessuna valutazione finora
- Faradic Foot BathDocumento16 pagineFaradic Foot BathMaansi Gupta100% (1)
- Nursing Lecture Blood PhysiologyDocumento90 pagineNursing Lecture Blood PhysiologyVSBNessuna valutazione finora
- ANA 6.01 General Somatic Afferents Dr. EsguerraDocumento22 pagineANA 6.01 General Somatic Afferents Dr. EsguerraNinna Ricci San JuanNessuna valutazione finora
- LMN VS UmnDocumento10 pagineLMN VS UmnyosuaNessuna valutazione finora
- Physiotherapy For Cardiac SurgeryDocumento15 paginePhysiotherapy For Cardiac SurgeryMuruganNessuna valutazione finora
- Electrotherapy: Laws and Theories in ElectrotherapyDocumento11 pagineElectrotherapy: Laws and Theories in ElectrotherapyEloisa100% (1)
- Development of GITDocumento88 pagineDevelopment of GITBindiya MangarNessuna valutazione finora
- Complications of Bed RestDocumento51 pagineComplications of Bed Restsuderson100% (1)
- Physiology of Hearing: Departemen Fisiologi FK UsuDocumento28 paginePhysiology of Hearing: Departemen Fisiologi FK UsuSonia P SNessuna valutazione finora
- Tumor OtakDocumento17 pagineTumor Otakmona030988Nessuna valutazione finora
- Cerebellar DisordersDocumento29 pagineCerebellar DisordersArslan Aslam100% (1)
- Chapter 1 - The Neurologic Examination: Section 3Documento15 pagineChapter 1 - The Neurologic Examination: Section 3gus_lionsNessuna valutazione finora
- General Neurological Assessment: Shemjaz Arakkal MDocumento54 pagineGeneral Neurological Assessment: Shemjaz Arakkal MRaghu NadhNessuna valutazione finora
- JURISprudence ReviewerDocumento30 pagineJURISprudence ReviewerVerlette Roselle Aguisanda Lizardo100% (1)
- People Vs CondesDocumento22 paginePeople Vs CondesVerlette Roselle Aguisanda LizardoNessuna valutazione finora
- Malacañan Palace Manila: March 7, 1979Documento3 pagineMalacañan Palace Manila: March 7, 1979Verlette Roselle Aguisanda LizardoNessuna valutazione finora
- GR 107789Documento36 pagineGR 107789Verlette Roselle Aguisanda LizardoNessuna valutazione finora
- 8910Documento61 pagine8910Verlette Roselle Aguisanda LizardoNessuna valutazione finora
- Chapter 14Documento27 pagineChapter 14Verlette Roselle Aguisanda LizardoNessuna valutazione finora
- Cardiovascular Control: Marinette Rumusud-Jambaro, MD Diplomate in Internal MedicineDocumento48 pagineCardiovascular Control: Marinette Rumusud-Jambaro, MD Diplomate in Internal MedicineVerlette Roselle Aguisanda LizardoNessuna valutazione finora
- Cessna 2Documento20 pagineCessna 2Janki KaushalNessuna valutazione finora
- Bristle Blaster BrochureDocumento12 pagineBristle Blaster BrochureAZLAN ABDULLAINessuna valutazione finora
- Sintering and Reduction Via Hydrogen of Egyptian Iron Ore Briquettes With Dolomite1Documento16 pagineSintering and Reduction Via Hydrogen of Egyptian Iron Ore Briquettes With Dolomite1Frederik RareNessuna valutazione finora
- 2.1) Instruction Manual (Sau8810) For Alarm Monitoring System - 6N-2521-102Documento50 pagine2.1) Instruction Manual (Sau8810) For Alarm Monitoring System - 6N-2521-102D ArsenNessuna valutazione finora
- MSA Training PPT 14-07-2020 PDFDocumento125 pagineMSA Training PPT 14-07-2020 PDFLAKSHYA MITTAL100% (4)
- IS 513 Grade EDDDocumento2 pagineIS 513 Grade EDDRamji GautamNessuna valutazione finora
- Prototype of Cansat With Auto-Gyro Payload For Small Satellite EducationDocumento7 paginePrototype of Cansat With Auto-Gyro Payload For Small Satellite EducationPusapati Saketh Varma ed21b048Nessuna valutazione finora
- The Mechanisms of Muscle Hypertrophy and Their Application To Resistance TrainingDocumento17 pagineThe Mechanisms of Muscle Hypertrophy and Their Application To Resistance TrainingSurama SilvaNessuna valutazione finora
- Nonlinear Dynamic Matrix Control For Hig PDFDocumento12 pagineNonlinear Dynamic Matrix Control For Hig PDFMMHFNessuna valutazione finora
- Sam Woods Prompt PlaybookDocumento48 pagineSam Woods Prompt PlaybookhagaiNessuna valutazione finora
- Contribution of AryabhattaDocumento14 pagineContribution of AryabhattaMd yaqub71% (14)
- EI 1 (Chapter 3)Documento42 pagineEI 1 (Chapter 3)Getachew RaboNessuna valutazione finora
- An Investigation On Gas Lift Performance Curve in An Oil Producing Well (Deni Saepudin)Documento16 pagineAn Investigation On Gas Lift Performance Curve in An Oil Producing Well (Deni Saepudin)Atrian RahadiNessuna valutazione finora
- A Novel Meta-Heuristic Approach For Load Balancing in Cloud ComputingDocumento9 pagineA Novel Meta-Heuristic Approach For Load Balancing in Cloud ComputingPraveen Kumar UmmidiNessuna valutazione finora
- Leerhoekie - Lockdown Freebie - Maths GR 3Documento16 pagineLeerhoekie - Lockdown Freebie - Maths GR 3NonhlakaniphoNessuna valutazione finora
- Bey Hakim Taz Temporary Autonomous ZoneDocumento17 pagineBey Hakim Taz Temporary Autonomous ZoneAna RibeiroNessuna valutazione finora
- Linear Equations in One VariableDocumento10 pagineLinear Equations in One VariableRiddhiman BoseNessuna valutazione finora
- Imperfections 1Documento26 pagineImperfections 1Mugunthan KrishnaNessuna valutazione finora
- LA3450Documento16 pagineLA3450costi theodoruNessuna valutazione finora
- Mark The Letter A, B, C, or D On Your Answer Sheet To Indicate The Correct Answer To Each of The Following QuestionsDocumento44 pagineMark The Letter A, B, C, or D On Your Answer Sheet To Indicate The Correct Answer To Each of The Following QuestionsPhạm Trần Gia HuyNessuna valutazione finora
- Os Assignment: 1. Write A Program in JAVA For FCFS CPU Scheduling. CODEDocumento7 pagineOs Assignment: 1. Write A Program in JAVA For FCFS CPU Scheduling. CODESoumya Ranjan BeheraNessuna valutazione finora
- Intelligent Variable Speed Pumps: Solution OutlineDocumento12 pagineIntelligent Variable Speed Pumps: Solution OutlineArjun ReddyNessuna valutazione finora
- Topic 1 - Basic Reading SkillsDocumento35 pagineTopic 1 - Basic Reading SkillsWyn Kristle DuterteNessuna valutazione finora
- THEORIES OF TRUTH Intro To Philo 3rd WeekDocumento14 pagineTHEORIES OF TRUTH Intro To Philo 3rd WeekChelsea GraceNessuna valutazione finora
- Plate Tectonics Gizmo Form PDFDocumento5 paginePlate Tectonics Gizmo Form PDFJorge Cota85% (13)
- A Review On Liquid-Phase Exfoliation For Scalable Production of Pure Graphene, PDFDocumento94 pagineA Review On Liquid-Phase Exfoliation For Scalable Production of Pure Graphene, PDFShofwa AnnisaaNessuna valutazione finora
- Module 2 Ethics and Culture-3Documento26 pagineModule 2 Ethics and Culture-3Charles Ronald GenatoNessuna valutazione finora
- Math Cheat SheetsDocumento64 pagineMath Cheat SheetsSubrata Das100% (1)
- 3rd Green Building MasterplanDocumento16 pagine3rd Green Building MasterplantatonyNessuna valutazione finora
- Anthropology and The Changing WorldDocumento12 pagineAnthropology and The Changing Worldbilal1710Nessuna valutazione finora