Potrebbero piacerti anche
- Infectious Arthritides: Presenter Shamsa Yahya Supervisor DR Migowa 22/7/2019Documento28 pagineInfectious Arthritides: Presenter Shamsa Yahya Supervisor DR Migowa 22/7/2019Felix Wafula MusibiNessuna valutazione finora
- Bones Joint InfectionsDocumento28 pagineBones Joint InfectionsPrincewill SeiyefaNessuna valutazione finora
- Pediatric Septic Arthritis: Nicole I. Montgomery,, Howard R. EppsDocumento8 paginePediatric Septic Arthritis: Nicole I. Montgomery,, Howard R. EppsnormasusanaNessuna valutazione finora
- Grade 2 InfectionDocumento29 pagineGrade 2 InfectionshaifNessuna valutazione finora
- Prof. Beata Sobieszczańska Wrocław Medical University Dept. of MicrobiologyDocumento44 pagineProf. Beata Sobieszczańska Wrocław Medical University Dept. of MicrobiologyBeata SobieszczańskaNessuna valutazione finora
- Lymph Ad en Op A ThyDocumento24 pagineLymph Ad en Op A ThyAlyaa El SayedNessuna valutazione finora
- Bone and Joint InfectionDocumento78 pagineBone and Joint InfectionMahmoud Abu Al AmrainNessuna valutazione finora
- Pediatric Septic Arthritis: Nicole I. Montgomery,, Howard R. EppsDocumento8 paginePediatric Septic Arthritis: Nicole I. Montgomery,, Howard R. EppsIvanNessuna valutazione finora
- Fungal Infections in Diabetes Mellitus: An Overview: Review ArticleDocumento5 pagineFungal Infections in Diabetes Mellitus: An Overview: Review ArticleAudrey Ira YunitaNessuna valutazione finora
- Bacterial and Viral Infection in ChildrenDocumento62 pagineBacterial and Viral Infection in ChildrenislawatiNessuna valutazione finora
- 2023.pedia - Trans24.-Bacterial-Infections - Gram Postitive (Part 1)Documento6 pagine2023.pedia - Trans24.-Bacterial-Infections - Gram Postitive (Part 1)Adrian CaballesNessuna valutazione finora
- Orthopaedic InfectionsDocumento6 pagineOrthopaedic InfectionsSurgicalgownNessuna valutazione finora
- OsteomilitisDocumento43 pagineOsteomilitisZelalem AbrhamNessuna valutazione finora
- Meningitis 4th Year FinalDocumento85 pagineMeningitis 4th Year FinalFawad JanNessuna valutazione finora
- Etiology: Acute Hematogenous Osteomyelitis Subacute Osteomyelitis Chronic OsteomyelitisDocumento42 pagineEtiology: Acute Hematogenous Osteomyelitis Subacute Osteomyelitis Chronic OsteomyelitisNoe-pal DynmNessuna valutazione finora
- Important Terms - Tropical InfectionDocumento8 pagineImportant Terms - Tropical InfectionTimothy JordanNessuna valutazione finora
- Aileen Ancla Elorde, MD, MCHM, DPPS, DPSAAI Child and Adult Allergy, Asthma, and ImmunologyDocumento67 pagineAileen Ancla Elorde, MD, MCHM, DPPS, DPSAAI Child and Adult Allergy, Asthma, and ImmunologyCarlBuscatoNessuna valutazione finora
- Bone and Joint InfectionsDocumento43 pagineBone and Joint InfectionsaugyeraNessuna valutazione finora
- Mikroorganisme Penyebab Infeksi Pada Sistem Reproduksi2003Documento132 pagineMikroorganisme Penyebab Infeksi Pada Sistem Reproduksi2003anitacharisNessuna valutazione finora
- Micro Final Buzz Word CheatsheetDocumento10 pagineMicro Final Buzz Word CheatsheetThesmith FamNessuna valutazione finora
- Bone & Joint Infections For Wurh c1Documento26 pagineBone & Joint Infections For Wurh c1SeyfNessuna valutazione finora
- Catatan b15m4Documento18 pagineCatatan b15m4Vivi ArsiNessuna valutazione finora
- Thoracicinfectionsin Immunocompromisedpatients: Jitesh Ahuja,, Jeffrey P. KanneDocumento16 pagineThoracicinfectionsin Immunocompromisedpatients: Jitesh Ahuja,, Jeffrey P. KanneMateoNessuna valutazione finora
- Bone and Joint InfectionDocumento43 pagineBone and Joint Infectionraheeg siddigNessuna valutazione finora
- Infection Related GNDocumento9 pagineInfection Related GN8ctvnvpbnpNessuna valutazione finora
- Evaluation of The Immune SystemDocumento17 pagineEvaluation of The Immune SystemDrshadiNessuna valutazione finora
- Absolute Neutrophil CountDocumento4 pagineAbsolute Neutrophil Countsmckenzie1964Nessuna valutazione finora
- Opportunistic Infections PDFDocumento88 pagineOpportunistic Infections PDFironbuang100% (1)
- Orthopedic Infections, Osteomyelitis:Septic ArthritisDocumento65 pagineOrthopedic Infections, Osteomyelitis:Septic ArthritisnhfbyqvgwhNessuna valutazione finora
- 9.pneumonia 1 Nov '19Documento62 pagine9.pneumonia 1 Nov '19Arleen MatincaNessuna valutazione finora
- Joint InfectionsDocumento10 pagineJoint InfectionsJPNessuna valutazione finora
- Skin and Soft-Tissue Infections: ImpetigoDocumento26 pagineSkin and Soft-Tissue Infections: ImpetigoDr. Rizwanuddin QaziNessuna valutazione finora
- Referat Lisa (Anestesi)Documento32 pagineReferat Lisa (Anestesi)Lisa Raihan LutfiaNessuna valutazione finora
- Infections of The Digestive GlandsDocumento17 pagineInfections of The Digestive GlandsCrystal Lynn Keener SciariniNessuna valutazione finora
- Cardiovascular Infection - Etiology - AEP 2020 ElearnDocumento37 pagineCardiovascular Infection - Etiology - AEP 2020 ElearnLaura DelinusNessuna valutazione finora
- Infectious Disease and Lymphoreticular SystemDocumento26 pagineInfectious Disease and Lymphoreticular Systemseptian_tjayaNessuna valutazione finora
- Bone and Joint InfectionsDocumento52 pagineBone and Joint Infectionsabenezer g/kirstosNessuna valutazione finora
- Mikrobiologi URODocumento154 pagineMikrobiologi UROSyifa Aulia Fatimah BashariNessuna valutazione finora
- Netter's Internal Medicine 2nd Ed 17Documento19 pagineNetter's Internal Medicine 2nd Ed 17Panagiotis SouldatosNessuna valutazione finora
- Bone Infections in Children Are Important Because of Their Potential To Cause Permanent DisabilityDocumento8 pagineBone Infections in Children Are Important Because of Their Potential To Cause Permanent DisabilityNavjot SoochNessuna valutazione finora
- BM 2.3 Bambang SudarmantoDocumento46 pagineBM 2.3 Bambang SudarmantoAbdullah ShiddiqNessuna valutazione finora
- Mss InfectionDocumento41 pagineMss InfectionZelalem AbrhamNessuna valutazione finora
- M.O. Penyebab Arthritis, Osteomyelitis, Myo-Pericarditis (Prof - Dr.efrida)Documento35 pagineM.O. Penyebab Arthritis, Osteomyelitis, Myo-Pericarditis (Prof - Dr.efrida)Rizki ArvianantaNessuna valutazione finora
- Siu Empiric Antibiotics For Select InfectionsDocumento30 pagineSiu Empiric Antibiotics For Select InfectionspasswordNessuna valutazione finora
- Osteomyelitis2 200610201550Documento46 pagineOsteomyelitis2 200610201550Lolo Toto100% (1)
- Presentation 1Documento13 paginePresentation 1Zeinab AliNessuna valutazione finora
- Septic Arthritis Characterized byDocumento55 pagineSeptic Arthritis Characterized byNdor BariboloNessuna valutazione finora
- Resistance Phenotypic of GramDocumento25 pagineResistance Phenotypic of GramProiectulTauNessuna valutazione finora
- Septic ArthritisDocumento6 pagineSeptic ArthritisJayricDepalobosNessuna valutazione finora
- Septic ArthritisDocumento32 pagineSeptic ArthritisDr. BosotovNessuna valutazione finora
- Congenital Infections - Dr. R. Adhi Teguh SpA (K)Documento65 pagineCongenital Infections - Dr. R. Adhi Teguh SpA (K)syak turNessuna valutazione finora
- Lec8 Infectious DiseasesDocumento32 pagineLec8 Infectious DiseasesmanuelNessuna valutazione finora
- Septic Arthritis: A Diagnosis Not To Be MissedDocumento5 pagineSeptic Arthritis: A Diagnosis Not To Be MissedJHERY LIMAYMANTA GONZALESNessuna valutazione finora
- Osteomyelitis: Acute & ChronicDocumento35 pagineOsteomyelitis: Acute & ChronicrainakenovNessuna valutazione finora
- Invasive Fungal InfectionsDocumento55 pagineInvasive Fungal InfectionsPrincewill SmithNessuna valutazione finora
- A. Introduction of Skin and Soft Tissue InfectionsDocumento10 pagineA. Introduction of Skin and Soft Tissue InfectionsChristin alexaNessuna valutazione finora
- Flaviviridae NewDocumento25 pagineFlaviviridae NewHafsah G.Nessuna valutazione finora
- Child Presenting With Joint PainDocumento22 pagineChild Presenting With Joint PainlagathurcNessuna valutazione finora
- Neonatal Surgical InfectionDocumento43 pagineNeonatal Surgical InfectionAhmad Abu KushNessuna valutazione finora
- Leonardi A. GoenawanDocumento33 pagineLeonardi A. GoenawanJaneNessuna valutazione finora
- Introduction To Biochemistry: Rondang Soegianto 2009Documento11 pagineIntroduction To Biochemistry: Rondang Soegianto 2009JaneNessuna valutazione finora
- Signal Transduction: Rondang R. Soegianto 2009Documento21 pagineSignal Transduction: Rondang R. Soegianto 2009JaneNessuna valutazione finora
- Gastrointestinal System: Digestion and Absorption of NutrientsDocumento49 pagineGastrointestinal System: Digestion and Absorption of NutrientsJaneNessuna valutazione finora
- Enzymes and Substrates: Rondang R. SoegiantoDocumento19 pagineEnzymes and Substrates: Rondang R. SoegiantoJaneNessuna valutazione finora
- Chemistry of Major Compounds in The Body: Carbohydrates Lipids Proteins Nucleic AcidsDocumento28 pagineChemistry of Major Compounds in The Body: Carbohydrates Lipids Proteins Nucleic AcidsJaneNessuna valutazione finora
- COVID-19 Vaccine Study Reveals Myocarditis Cases in The U.S. MilitaryDocumento4 pagineCOVID-19 Vaccine Study Reveals Myocarditis Cases in The U.S. MilitaryJeffery TaylorNessuna valutazione finora
- Tuberculosis BCG VaccineDocumento16 pagineTuberculosis BCG VaccineQworldNessuna valutazione finora
- Doktersverklaring EngelsDocumento1 paginaDoktersverklaring EngelsSl IMNessuna valutazione finora
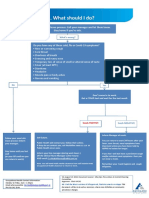
- What To Do If Youre Sick FlowchartDocumento1 paginaWhat To Do If Youre Sick FlowchartfuckyouNessuna valutazione finora
- CertificateDocumento1 paginaCertificateparnapasuNessuna valutazione finora
- Methodological Instructions - Module 2Documento60 pagineMethodological Instructions - Module 2Frt TrfNessuna valutazione finora
- HIV - Global HIV Neurology - A Comprehensive Review - 2018Documento2 pagineHIV - Global HIV Neurology - A Comprehensive Review - 2018Juan Salazar PajaresNessuna valutazione finora
- Bacteriology Edited 1Documento65 pagineBacteriology Edited 1Ali AhmedNessuna valutazione finora
- Iga Afifah Rahmadini 20420020 Intervensi WabahDocumento17 pagineIga Afifah Rahmadini 20420020 Intervensi WabahIga AfifahNessuna valutazione finora
- HSE Bulletin # 84: Break The Chain of Corona Virus Transmission Stay Safe & Stay at HomeDocumento1 paginaHSE Bulletin # 84: Break The Chain of Corona Virus Transmission Stay Safe & Stay at HomeAbdus SamadNessuna valutazione finora
- Assessment Dianosis Planning Intervention Rationale EvaluationDocumento2 pagineAssessment Dianosis Planning Intervention Rationale Evaluationkyaw100% (1)
- Bfp9 Health Declaration FormDocumento1 paginaBfp9 Health Declaration FormGelli Jane GurdielNessuna valutazione finora
- Handout CompilationDocumento199 pagineHandout CompilationG Fab100% (2)
- LAS Q3-Health8-Week-6-8Documento8 pagineLAS Q3-Health8-Week-6-8novem salonoyNessuna valutazione finora
- Clarithromycin Drug StudyDocumento1 paginaClarithromycin Drug StudyJanine Joy Orpilla100% (4)
- Antibiotic Prophylaxis OrthoDocumento4 pagineAntibiotic Prophylaxis OrthoDonNessuna valutazione finora
- 2020-3P-Mycoplasma PneumoniaeDocumento18 pagine2020-3P-Mycoplasma PneumoniaeSin SeutNessuna valutazione finora
- Acute Flaccid Paralysis Surveillance PDFDocumento1 paginaAcute Flaccid Paralysis Surveillance PDFMutiara DewiNessuna valutazione finora
- Old Disease NamesDocumento52 pagineOld Disease NamesMuhammad Ata Ul MustafaNessuna valutazione finora
- Ams Ipc SlidesDocumento36 pagineAms Ipc SlidesHarriet TembaNessuna valutazione finora
- Cholera ARDocumento6 pagineCholera ARImmanuelNessuna valutazione finora
- Artron COVID-19 Ab Report 20200317 PDFDocumento7 pagineArtron COVID-19 Ab Report 20200317 PDFMusaMirNessuna valutazione finora
- Nhs Covid Pass - Vaccinated: Pfizer/Biontech Covid-19 Vaccine Pfizer/Biontech Covid-19 VaccineDocumento1 paginaNhs Covid Pass - Vaccinated: Pfizer/Biontech Covid-19 Vaccine Pfizer/Biontech Covid-19 VaccinePscual OuramdaneNessuna valutazione finora
- XBB.1.5: A New Threatening SARS-CoV-2 Omicron SubvariantDocumento4 pagineXBB.1.5: A New Threatening SARS-CoV-2 Omicron SubvariantAminul IslamNessuna valutazione finora
- ASL Project by Ansh Semwal XII - S2Documento25 pagineASL Project by Ansh Semwal XII - S2KESHAV VARSHNEYNessuna valutazione finora
- Parasitic ArthropodsDocumento3 pagineParasitic ArthropodsVicky V. HerpworldNessuna valutazione finora
- Hepatitis B VaccineDocumento3 pagineHepatitis B VaccineChoox PriiNessuna valutazione finora
- The Most Dangerous in HistoryDocumento10 pagineThe Most Dangerous in HistorymausanpraNessuna valutazione finora
- Tylomix 250 Tylosine Feed PremixDocumento1 paginaTylomix 250 Tylosine Feed PremixLalit ChaudhariNessuna valutazione finora
- C. DiffDocumento20 pagineC. DiffVijay Agrawal100% (1)