Potrebbero piacerti anche
- Fast Facts: Respiratory Allergies: Understand aeroallergens, improve treatment responseDa EverandFast Facts: Respiratory Allergies: Understand aeroallergens, improve treatment responseNessuna valutazione finora
- Obstructive Airway and Pulmonary Disease - Dr. Ahmad RasyidDocumento95 pagineObstructive Airway and Pulmonary Disease - Dr. Ahmad Rasyidanisia ayundaNessuna valutazione finora
- Asthma: A. DefinitionDocumento6 pagineAsthma: A. DefinitionElvando SimatupangNessuna valutazione finora
- AsmaDocumento39 pagineAsmaAndi ZultasyriqNessuna valutazione finora
- 10th Tutorial - Asthma Bronchiale WebDocumento75 pagine10th Tutorial - Asthma Bronchiale WebFety FatimahNessuna valutazione finora
- AsthmaDocumento66 pagineAsthmaapi-3729824100% (4)
- AsmaDocumento34 pagineAsmaRiselena Alyssa AmaDheaNessuna valutazione finora
- Supplementary Material 1a Acute AsthmaDocumento3 pagineSupplementary Material 1a Acute AsthmaANGELIE CRISTINE POMADONessuna valutazione finora
- Supplementary Material 1a Acute AsthmaDocumento3 pagineSupplementary Material 1a Acute AsthmaJanela Chriselle B. TICARNessuna valutazione finora
- Asma Bronkiale: Muhsin Ppds Ilmu Penyakit Dalam FK Unsyiah Pembimbing: Dr. T. Mamfaluti, M.Kes, SP - PD, FinasimDocumento33 pagineAsma Bronkiale: Muhsin Ppds Ilmu Penyakit Dalam FK Unsyiah Pembimbing: Dr. T. Mamfaluti, M.Kes, SP - PD, FinasimEvy LiesniawatiNessuna valutazione finora
- Asthma: Presentation By: Dr. Zunaira Nawaz Dr. Nida ShafiqueDocumento47 pagineAsthma: Presentation By: Dr. Zunaira Nawaz Dr. Nida ShafiqueMohammad AliNessuna valutazione finora
- Obstructive Pulmonary DiseasesDocumento50 pagineObstructive Pulmonary DiseasesGopala HariNessuna valutazione finora
- Asthma Bronchiale: Dr. Ramelan Navy Hospital SurabayaDocumento53 pagineAsthma Bronchiale: Dr. Ramelan Navy Hospital SurabayaCornelia CindyNessuna valutazione finora
- 4 AsthmaDocumento32 pagine4 AsthmaSalman KhanNessuna valutazione finora
- Dr. Ediyono SP P Sub Dep Paru RSAL DR Ramelan: UHT September 2012Documento50 pagineDr. Ediyono SP P Sub Dep Paru RSAL DR Ramelan: UHT September 2012gabyNessuna valutazione finora
- AsthmaDocumento44 pagineAsthmaEmmaNessuna valutazione finora
- Asma Bronchiale: Dr. Budi ShanjayaDocumento29 pagineAsma Bronchiale: Dr. Budi ShanjayaDesi PhykiNessuna valutazione finora
- Web 24 - Teti Madiadipoera - Treatment and Management of Rhinitis AllergyDocumento38 pagineWeb 24 - Teti Madiadipoera - Treatment and Management of Rhinitis AllergyEdzhar HasiholanNessuna valutazione finora
- Asma BronkialDocumento27 pagineAsma BronkialTa'byObheNessuna valutazione finora
- Asma Pada AnakDocumento24 pagineAsma Pada AnaksevyarvintaNessuna valutazione finora
- Dr. Sak Indriyani, Spa, Mkes: Department of Child Health Rsu MataramDocumento48 pagineDr. Sak Indriyani, Spa, Mkes: Department of Child Health Rsu MataramMuhammad Bilal Bin AmirNessuna valutazione finora
- Integrated Therapeutics IiiDocumento91 pagineIntegrated Therapeutics IiiSalahadinNessuna valutazione finora
- ASTHMADocumento26 pagineASTHMALe RobertNessuna valutazione finora
- Bronchial AsthmaDocumento11 pagineBronchial AsthmaVishva Lalitbhai Hirpara100% (1)
- Pharmacology 312: Assignment 3: Respiratory DiseasesDocumento5 paginePharmacology 312: Assignment 3: Respiratory DiseasesTerepe CrimsonNessuna valutazione finora
- Lecture 06. Bronchial AsthmaDocumento30 pagineLecture 06. Bronchial AsthmaJavier SaadNessuna valutazione finora
- Allergic RhinitisDocumento55 pagineAllergic RhinitisZZNessuna valutazione finora
- Asma Current Family MedicineDocumento7 pagineAsma Current Family MedicineRay Erick RamosNessuna valutazione finora
- Journal Reading Allergic RhinitisDocumento39 pagineJournal Reading Allergic RhinitisBimaKharismaNessuna valutazione finora
- Asthma by Ikmal WahabDocumento19 pagineAsthma by Ikmal WahabIkmal WahabNessuna valutazione finora
- Asthma Management: Abdul Moeloek General HospitalDocumento37 pagineAsthma Management: Abdul Moeloek General HospitalCaesarioNessuna valutazione finora
- Anaphylaxis: DR - Arvinth SoundarrajanDocumento26 pagineAnaphylaxis: DR - Arvinth SoundarrajanP Vinod KumarNessuna valutazione finora
- NCM-112-RESP (Sanaani, Nur-Fatima, M.) (Drug Study)Documento2 pagineNCM-112-RESP (Sanaani, Nur-Fatima, M.) (Drug Study)Nur SetsuNessuna valutazione finora
- Diagnosis Rinitis AlergiDocumento42 pagineDiagnosis Rinitis AlergiRaymond NadeakNessuna valutazione finora
- Asthma Bronchiale: Ns. Kasmawati, S.Kep.M.KepDocumento35 pagineAsthma Bronchiale: Ns. Kasmawati, S.Kep.M.KepSari YanaNessuna valutazione finora
- Bronchial AsthmaDocumento20 pagineBronchial AsthmaJuliet De GuzmanNessuna valutazione finora
- ASTHMADocumento41 pagineASTHMARobert L G MabongaNessuna valutazione finora
- Penatalaksanaan Asma: Sub Bag Alergi Imunologi Ilmu Penyakit Dalam FK Unsri/RSMH PalembangDocumento71 paginePenatalaksanaan Asma: Sub Bag Alergi Imunologi Ilmu Penyakit Dalam FK Unsri/RSMH PalembangAnityo NugrohoNessuna valutazione finora
- Asthma: DR Mayank Kumar MishraDocumento51 pagineAsthma: DR Mayank Kumar MishraMukesh ThakurNessuna valutazione finora
- Pharmacotherapy of AsthmaDocumento53 paginePharmacotherapy of AsthmaStella Aprilia NurNessuna valutazione finora
- Allergic RhinitisDocumento53 pagineAllergic RhinitisYousfNessuna valutazione finora
- Concept Map AsthmaDocumento3 pagineConcept Map AsthmaKaren HutchinsonNessuna valutazione finora
- Case Study Respiratory DisorderDocumento17 pagineCase Study Respiratory DisorderJester GalayNessuna valutazione finora
- Asthma Management: Abdul Moeloek General HospitalDocumento37 pagineAsthma Management: Abdul Moeloek General Hospitalkarina azlia amandaNessuna valutazione finora
- 20-05 Nebulization Neb AstraZeneca Pulmicort Steroid F Acute Asthma PRST - Dr. Darmawan - SharedDocumento60 pagine20-05 Nebulization Neb AstraZeneca Pulmicort Steroid F Acute Asthma PRST - Dr. Darmawan - SharedAndi MarsaliNessuna valutazione finora
- G IN A: Lobal Itiative For SthmaDocumento73 pagineG IN A: Lobal Itiative For SthmaKinasih Wahyu NingtyasNessuna valutazione finora
- Asma Anak - FIXDocumento54 pagineAsma Anak - FIXVIVI YULIYANINessuna valutazione finora
- NAPZA IntoksikasiDocumento46 pagineNAPZA IntoksikasiaprinalNessuna valutazione finora
- Nirmal Kumar Meena: Nursing Tutor, Aiims, JodhpurDocumento42 pagineNirmal Kumar Meena: Nursing Tutor, Aiims, JodhpurmalathiNessuna valutazione finora
- Asthma and COPDDocumento79 pagineAsthma and COPDDawit g/kidanNessuna valutazione finora
- БронхиальнаяDocumento51 pagineБронхиальнаяDaniel FunkNessuna valutazione finora
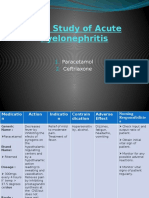
- Drug Study of Acute PyelonephritisDocumento6 pagineDrug Study of Acute PyelonephritisGhra CiousNessuna valutazione finora
- Status Asthmaticus: Triwahju AstutiDocumento41 pagineStatus Asthmaticus: Triwahju AstutirianiNessuna valutazione finora
- Topic: Asthma and Copd: Internal Medicine IiDocumento8 pagineTopic: Asthma and Copd: Internal Medicine IicarlosNessuna valutazione finora
- (KULIAH 5) Reaksi AnafilaksisDocumento30 pagine(KULIAH 5) Reaksi AnafilaksisArtawa Darma YudaNessuna valutazione finora
- Anaphylaxis: Prof. Rusudan KarseladzeDocumento21 pagineAnaphylaxis: Prof. Rusudan KarseladzepalNessuna valutazione finora
- Asma AnakDocumento53 pagineAsma AnakAsri Rasyid LaskarIRDNessuna valutazione finora
- Curriculum Vitae: Dr. Muh - Ilyas, SP - PD, KP, SP.P (K), FINASIMDocumento51 pagineCurriculum Vitae: Dr. Muh - Ilyas, SP - PD, KP, SP.P (K), FINASIMMuhammad ZakkiNessuna valutazione finora
- Asthma 01Documento74 pagineAsthma 01Dian zaini PutraNessuna valutazione finora
- Allergic & VasomotoDocumento60 pagineAllergic & VasomotoDilip BiswasNessuna valutazione finora
- Petcare Power of AttorneyDocumento4 paginePetcare Power of AttorneyLisaHospetsNessuna valutazione finora
- Part III Internal Medicine Examination AnswersDocumento91 paginePart III Internal Medicine Examination AnswersFırat GüllüNessuna valutazione finora
- CVBD Easy-To-Digest No 4 BabesiosisDocumento12 pagineCVBD Easy-To-Digest No 4 BabesiosisDocNessuna valutazione finora
- DEV2011 2018 Practical Week 8 DRAFT REPORT PDFDocumento1 paginaDEV2011 2018 Practical Week 8 DRAFT REPORT PDFAreesha FatimaNessuna valutazione finora
- Journal Pone 0208697 PDFDocumento14 pagineJournal Pone 0208697 PDFRenzo Flores CuadraNessuna valutazione finora
- Dental ImplantsDocumento1 paginaDental ImplantsPaWan VelagaNessuna valutazione finora
- Bipolar Disorder Journal Reading (International Journal Research of Pharmacy)Documento19 pagineBipolar Disorder Journal Reading (International Journal Research of Pharmacy)Imron RosyadiNessuna valutazione finora
- Urinary System and Disorders IntroductionDocumento23 pagineUrinary System and Disorders IntroductionHananya ManroeNessuna valutazione finora
- How A Diagnosis of Asperger's Transformed A Marriage: The Journal of Best Practices by David FinchDocumento24 pagineHow A Diagnosis of Asperger's Transformed A Marriage: The Journal of Best Practices by David FinchSimon and Schuster100% (10)
- My Hands The Body Is Painful / Do ROM Actions Done With MyDocumento3 pagineMy Hands The Body Is Painful / Do ROM Actions Done With MyHanip Little-FaqotNessuna valutazione finora
- Msds PG LyondellDocumento9 pagineMsds PG LyondellGia Minh Tieu TuNessuna valutazione finora
- 2018 Chapter 3-1 2018 Introduction To Industrial Higiene & Occupational Health PDFDocumento59 pagine2018 Chapter 3-1 2018 Introduction To Industrial Higiene & Occupational Health PDFLove StrikeNessuna valutazione finora
- AARC Clinical Practice GuidelineDocumento7 pagineAARC Clinical Practice GuidelineXime GonzálezNessuna valutazione finora
- Jrsocmed00158 0011 PDFDocumento6 pagineJrsocmed00158 0011 PDFWahyu SutrisnaNessuna valutazione finora
- Analice Mendel: Clinical Doctorate in Occupational Therapy GPA: 4.0Documento1 paginaAnalice Mendel: Clinical Doctorate in Occupational Therapy GPA: 4.0api-518311936Nessuna valutazione finora
- There Is Good News For Coffee LoversDocumento5 pagineThere Is Good News For Coffee Loversfirsty marthaNessuna valutazione finora
- Patofisiologi Kanker RahimDocumento98 paginePatofisiologi Kanker RahimOjo Nesu100% (1)
- OMG 6 Sains TG 5 - Bab 01Documento15 pagineOMG 6 Sains TG 5 - Bab 01Azizah EmbongNessuna valutazione finora
- Health and H BehaviorDocumento69 pagineHealth and H BehaviorDawud AsnakewNessuna valutazione finora
- Journal Homepage: - : IntroductionDocumento8 pagineJournal Homepage: - : IntroductionIJAR JOURNALNessuna valutazione finora
- NAVLE Study Strategies Zuku ReviewDocumento60 pagineNAVLE Study Strategies Zuku ReviewMohamed Omar90% (10)
- SSOPDocumento133 pagineSSOPYanuar Rufianti Wongi100% (1)
- Npte Exam TablesDocumento586 pagineNpte Exam TablesarbazNessuna valutazione finora
- Practice Guidelines For Obstetric Anesthesia An Updated Report by The American Society of Anesthesiologists Task Force On Obstetric AnesthesiaDocumento14 paginePractice Guidelines For Obstetric Anesthesia An Updated Report by The American Society of Anesthesiologists Task Force On Obstetric AnesthesiaMadalina TalpauNessuna valutazione finora
- Neurology II 6.04 Traumatic Brain Injury Dr. TanDocumento10 pagineNeurology II 6.04 Traumatic Brain Injury Dr. TanAbi IgsNessuna valutazione finora
- Health and WellnessDocumento59 pagineHealth and Wellnessvenkata karthikNessuna valutazione finora
- Review Article: The Onstep Method For Inguinal Hernia Repair: Operative Technique and Technical TipsDocumento8 pagineReview Article: The Onstep Method For Inguinal Hernia Repair: Operative Technique and Technical TipsKaterina TsNessuna valutazione finora
- The Blood of DraculaDocumento20 pagineThe Blood of DraculaJackSiedschlagNessuna valutazione finora
- Language and The BrainDocumento8 pagineLanguage and The BrainAntonio GoqueNessuna valutazione finora
- LCB Surgical Technique - 2022 Update v3Documento24 pagineLCB Surgical Technique - 2022 Update v3Samuel SalvadorNessuna valutazione finora